I'm assuming that these decisions aren't political and are genuinely being taken for medical reasons. I mean, I sure hope so.
The big impact is not a few days of delay. The big impact is the loss of trust in this vaccine in the general populace.
> I'm assuming that these decisions aren't political and are genuinely being taken for medical reasons. I mean, I sure hope so.
Obvious disclaimer: I'm not a medical expert.
However, I wouldn't be so sure it's a wise decision. I primarily trust Karl Lauterbach's [1] opinion on these matters, and he is actively criticizing the move on Twitter as an overreaction [2].
[1] Karl Lauterbach is the director of an institute for epidemiology at a German university and also a member of the German Federal parliament for the Social Democrats (who are part of the current coalition).
[2] Source (in German): https://twitter.com/Karl_Lauterbach/status/13714710614018949...
Not that I agree with the decision, but it's more complicated. People have to trust the vaccines to actually take them. There is already the fear that the process has been rushed, and particularly with AstraZeneca, there are some trust issues. Again, I don't want to argue that the concerns themselves are founded, just that they exists.
If that is the right measure to address those concerns is not purely medical or easily quantifiable. If you don't suspend it, would people still take the vaccine? Would they take the others?
Personally, since that is the case, I think one should stick with the facts. Be transparent about it, and try not to preempt whatever people may think. I would take it without a moment of hesitation, if I would be offered the opportunity.
One of the many unknowns about these vaccines is the length of time they give immunity, this can only be determined with confidence by looking at the data after a sufficient amount of time has passed. If the immunity only lasts for say 10-20 weeks, then getting it one week early, would mean the immunity goes away one week early as well. So in this case, I'm not sure there would be a major measurable impact. If the immunity lasts for say 50 weeks, that would be a different story.
> making it the latest of several European countries to hit pause
The article also cites the EMA, an EU institution, and notes:
> Several EU countries have called a halt to the AstraZeneca vaccine
Would you have them list each and every country individually? It seems, to me, that you're just complaining for the sake of complaining. Expect better of HN comments.
- Denmark
- Norway
- Ireland
- Netherlands
- Iceland
- Bulgaria
- Romania (only partly, see child comment)
Am I missing any?
Romania hasn't, only for specific lot numbers that were reported by Italy and Denmark as problematic.
Here you go then: https://www.iol.co.za/news/africa/drc-postpones-covid-19-vac...
Sigh
AstraZeneca: 13 Pulmonary embolisms Pfizer-BioNTech: 15 Pulmonary embolisms
They banned people from taking a vaccine that is very safe and effective.
Give people a choice.
Public health really hasn't been upfront with a lot, and their back and forth on a number of issues, while maintaining this air of authority is ultimately counter-productive to building trust.
Thirty cases of blood clotting out of five million. More people will die because they're not vaccinated.
And that's ignoring the fact that this may just be a statistical blip. There's a lot of diseases humans could catch, and sometimes there's going to be clusters.
German politicians said they're suspending vaccinations "out of an abundance of caution".
Given these numbers, we should continue to vaccinate out of an abundance of caution.
These people would refuse to board a rescue vessel because "it seems kind of unstable" and prefer to keep treading water.
In my opinion they're very much pandering to the large anti-vax populations of these countries.
On Monday Germany, Spain, Italy, and France were among those to suspend deployment of the vaccine, following similar moves made last week by Denmark, Norway, Ireland, and others.
Thanksfully Germany acted now rationally, like the other countries. One idea would be to administer only half the dosis on younger people, as this was already tested, with much better results than with the full dosis. AZ is pretty strong, compared to the others.
I would not be surprised if this is simply a political and economic snub from the EU, one of very many the UK can expect over the coming decades.
The UK has spent the last half decade ENDLESSLY trying to score points against the EU on any and every topic. This sort of wrangling is part and parcel for the relationship the UK has chosen. Basically, if the current UK Government has gone anywhere NEAR this topic, don't expect the truth to linger. This certainly includes the chest-beating around the AZ vaccine, which the government were actually going to require be shipped with a fscking Union Flag on every vial.
Edit: My understanding was based around stories like this suggesting some delays, that AZ were "striving" to deliver, and more dosed being ordered after AZ testing not covering over 65s (at the time), some hesitancy, and general mud slinging. When I say "generally short" I guess I should say that I doubt even the chest-beating Brits will be fully two-dose vaccinated to 80-90% before Autumn. It's been a year and a month or two is second order optimization in my view.
If you are concerned about shortages, there are some other continents to consider first.
https://www.theguardian.com/world/2021/feb/24/astrazeneca-ex...
https://www.biopharma-reporter.com/Article/2021/02/18/EU-add...
https://www.nytimes.com/2021/02/25/world/europe/germany-coro...:
> Many people — including health workers — are skipping appointments or refusing to sign up for the AstraZeneca shot, which they fear is less effective than the Pfizer-BioNTech vaccine, the officials say. As a result, two weeks after the first delivery of 1.45 million doses of the AstraZeneca vaccine arrived in Germany, only 270,986 have been administered, according to data collected by the public health authority, the Robert Koch Institute.
Interesting that Twitter and Facebook also not labeling the concerns about AZ as "Fake News" so likely there is some merit to the claims against AZ.
I am also against taking AZ as well. If HN folks are confident it is fine go ahead. I will choose what I'm comfortable with and Germans or anybody else for that matter should have a say.
Let me correct that understanding. The EU is absolutely short on doses. AZ has only delivered 10% of what they promised. There is no doubt if the EU had a greater supply the vaccine rollout would be going much better.
The First stage is done in the US.
The second stage is done in the US and Germany.
The third stage is done in the US and Belgium.
[0] https://en.wikipedia.org/wiki/Pfizer–BioNTech_COVID-19_vacci...
- billions per week of half assed lockdown vs a few billion more for high quality timeley vaccine delivieries of the good stuff --- of course they chose the lockdown
- open schools as if nothing happens vs using UV-based air filtering machines and so on as a minimum level of precaution --- of course they choose to open schools with classrooms some of which even don't have windows that can be opened properly
- governing party members of parliament scamming the public out of money by selling overly expensive, low quality masks
- minister of health busy sueing newspapers for disclosing prices on his million dollar real estate purchases vs minister of health actually being busy 24/7 with fighting the crisis
the list goes "on and on and on", these are just the most popular ones right now. It's just a dumpster fire at this point and the positives will not be recognized divorced from said pile of crap.
This is not the issue. A few billion would not have magically solved the problems with vaccine deliveries. The EU has contracts with pharmaceutical companies which these companies are not honoring sometimes intentionally so.
AstraZeneca for example doesn't have the production capacity to supply what they promised to the EU even if the Belgian site was working properly. That's the result of the EU audit. These companies are betting that the consequence of them not fullfiling their contractual obligation will be insignificant compared to their benefits. As these companies remain hugely profitable, their production issue is not linked to difficulty accessing capital. It is naive to assume things would have gone differently if the EU was paying more. It would just have meant more profits for them.
The heart of the issue is that contraty to the USA or China the EU is weak so companies don't hesitate trampling it. If a Chinese company did to China what AstraZeneca is doing to the EU, the CCP would take control of it and its CEO would never be seen again. Meanwhile, the USA has little qualm using its legal system to punish companies defying the state to much. Congressional inquiries are not fun.
Any potential safety issues with vaccines must be investigated, otherwise there will be a huge problem with trust in vaccines and in the regulator. There's already a huge problem with vaccine skepticism, and vaccine fanatics are making things worse.
Which is what WHO and EMA are saying. But now that there’s panic, they’re not relevant anymore.
Polititians are stuck between trying to make the free-for-all phase as long as possible, but still look as though they did everything to help, so that they can win the next election.
Compared to the status of 11.03.2021, additional cases (as of Monday, 15.03.2021) have now been reported in Germany. In the analysis of the new data status, the experts of the Paul Ehrlich Institute now see a striking accumulation of a special form of very rare cerebral vein thrombosis (sinus vein thrombosis) in conjunction with a deficiency of blood platelets (thrombocytopenia) and bleeding in temporal proximity to vaccinations with the COVID-19 vaccine AstraZeneca.
Translated with www.DeepL.com/Translator (free version)
Cerebral venous sinus thrombosis presents with nonspecific symptoms (eg headaches). It can only be diagnosed with cerebral imaging of specific modalities (CT or MR brain venogram, expensive and specialised tests). From speaking to colleagues in the UK, their hospital system is quite overwhelmed and doctors are repurposed outside their field (eg surgeons looking after internal medicine patients). It is quite possible in the throes of a pandemic to be underestimating the incidence of this condition in the UK.
"The decision today is purely precautionary..." given this level of signal. We don't have details on the age groups involved and the normal rates expected but I can hazard a Fermi Estimate that the risk is minuscule compared to COVID-19 itself. I look forward to seeing the actual data in coming days/weeks. Precaution without downside is acceptable; this is not one of those cases, IMO. YMMV.
You don't know this at all - we don't know what age groups are affected here, and COVID is pretty much negligible in many younger age groups. It's best to wait for more data to come in before drawing any conclusions.
1. If holding off AstraZeneca vaccine does not affect vaccination rate during the investigation period, it is a prudent thing to do.
2. If vaccine rate is expected to drop, number of expected increase in death per day due to covid vs blood clog should be compared, if we were to minimize short term death.
3. More concerning is unknown effect that could take a long time to materialize. This is a tough call to make since any effect is only theoretical at this point.
For those jurisdictions like the UK, India, and Canada that continue recommending AstraZeneca, I'd suggest that COVID-19 vaccines are like beer; the best one is the one in front of you.
Or perhaps not, given that 2020 deaths in Germany were 985,145, only 4.85% higher than 2019, and only 3.2% higher than 2018 (and so basically in line with what we would expect from an aging society).
https://www.destatis.de/DE/Themen/Gesellschaft-Umwelt/Bevoel...
> Birth control pills can also cause thrombosis. So why is there all the fuss about the COVID-19 Vaccine AstraZeneca? It is true that for birth control pills thromboses, even with fatal outcome, are known as a very rare side effect. They are listed in the Summary of Product Characteristics (SmPC). The birth control pill is available only on prescription. Every woman must be informed of this risk by the prescribing physician. For the COVID-19 Vaccine AstraZeneca, there is currently a suspected very rare side effect of sinus vein thrombosis with accompanying platelet deficiency, sometimes fatal. It is not listed in the SmPC. The consideration of whether the vaccine can continue to be used even though it may cause this very rare side effect (if necessary, after this risk has been added to the SmPC) will be made at the European level by the European Medicines Agency (EMA) and at the national level by politicians. The procedure has been initiated.
Which sounds pretty clearly like bureaucratic CYA instead of an actual cost/benefit analysis that takes into account the excess deaths that are now being caused due to pausing the vaccine rollout.
"This potential side-effect is not listed in the SmPC so we need to pause vaccinations", ignoring the fact that hundreds of people are dying every day in Germany (https://www.google.com/search?q=germany+covid+case+fatality+...).
I've had elevated blood markers for clotting during covid-19, and now I hear of this.
I'm thinking of taking 75 mg aspirin, before and after the vaccine. On the other hand, the issue is the patients have low platelet count and I understand that this is the way aspirin reduces blod clotting.
So, do these patients have low platelet count because they had blod clots, or the other way around?
Afik, in the case of COVID-19, clotting is an autoimune issue, so perhaps the clotting is not something related to the astra Zeneca vaccine, but something about the immune response itself.
https://www.cdc.gov/coronavirus/2019-ncov/vaccines/safety/al...
[0]: https://www.wsj.com/articles/astrazeneca-warns-europe-of-lar...
Of course they are influenced by what they see in the news and questions by the government, but aren't a political player.
Adenovirus-induced thrombocytopenia: the role of von Willebrand factor and P-selectin in mediating accelerated platelet clearance
https://www.sciencedirect.com/science/article/pii/S000649712...
You can see the number of reported cases across Europe in the EUDRA Vigilance database (if you manage to get through the Oracle BI interface and if it doesn't error out)
https://www.ema.europa.eu/en/human-regulatory/research-devel...
I don't understand why AstraZeneca doesn't just say: yeah blood clots are a risk, incidence 1/100,000 and everyone can move on. Why does everything needs to be so politicized with this vaccine.
It is politicized because it effects more or less everyone on the planet and people are setup to take popular things and turn them into polarizing issues for political power in politicians and social capital for ordinary people. This is how a whole lot of people seek out happiness, by being "right" in their social circles, especially in a way that shows them as superior to large groups of others who are "wrong".
Social media preys intentionally or unintentionally on this human psychological vulnerability (can we get a CVE on the human psyche?) and every bit of media wants to sell you a compelling story so they stoke the flames of A/B conflicts.
The mass psychology/mythology/philosophy of the day is based around this crap and will turn anything into a "political" issue and people just generally aren't well educated enough to think independently or evaluate situations rationally on their own so they allow their reason to be driven by systems which are evolutionarily dependent on preying on addictive human behavior.
Thalidomide is the most well known example, but there are many others:
https://en.wikipedia.org/wiki/Lumiracoxib -- Approved in Europe, not the USA. Withdrawn from sales due to side effects.
https://en.wikipedia.org/wiki/Zimelidine -- Same.
https://en.wikipedia.org/wiki/Tolrestat -- Approved in Europe, failed stage 3 clinical in the USA
https://en.wikipedia.org/wiki/Rimonabant -- Approved in Europe, failed in the USA, withdrawn worldwide because the side effects were so bad.
As news about some countries pausing its deployment spread, the pressure rises on other countries to follow suit, as they weigh the risk of public mistrust.
If in the near future, public mistrust about this brand of vaccine climbs higher but confidence in other vaccines does not drop as much, then governments will benefit from having deferred deployment of this vaccine, and they may benefit further by suspending deployment of this vaccine entirely, even if the vaccine is entirely vindicated to be safe.
This outcome would be unfair for the manufacturer, but it would sacrifice this brand to preserve public trust. Public trust is a key factor in healthcare policy in societies where some healthcare participation is voluntary and elections can significantly influence policy priorities.
However, the findings of blood clotting alone would not have sufficed for this argument as they really should be no cause for concern at this point in time. The knee-jerk response of other countries on the other hand makes this reasoning much more valid. Something something self-fulfilling prophecy
I think so too, especially since AZ is one of the least effective ones available.
Is pulling the vaccine (with minimal evidence that it's causing issues) worse? How many people are going to turn down the AZ vaccine now, even if there's not actually an issue?
This is false. Problems with AstraZeneca has little to do with any other vaccine. They're engineered entirely differently and mechanisms of action are wildly different.
Source: https://www.axios.com/concern-republican-coronavirus-vaccine...
The number of people who got sick equals the base rate, so I really don't see how this could be the case.
I get that herd immunity won't occur if a significant proportion of population isn't immunized... but it still works on an individual basis.
It's less effective if the recipient believes the vaccine is ineffective or dangerous, and can make side effects more likely to occur (nocebo effect).
Maybe the risk for some specific groups justify giving them another vaccine?
[1]: https://apnews.com/article/germany-suspends-astrazeneca-vacc...
[1]: https://www.francetvinfo.fr/live/message/604/f7f/da5/ff4/e9f... (in French)
I would (and did) jump out of planes with a parachute recreationally, but if untrustworthy people started advocating it, proposing it should be mandatory, and unstable people dressed up in double flight suits in the streets started shaming others into doing it, I would definitely not jump out of planes anymore.
If it were true that the probability of complications/death from covid are heavily skewed to people over 75 and some obvious co-morbidities, we could vaccinate everyone in that risk group in a matter of weeks. What is the case for anyone who isn't a medical worker outside the real at-risk cohort to take on the endogenous risk of a vaccine? I could make one, but I'm more interested in what more knowledgeable people have to say about it, and judging by rising popular skepticism, we're going to need one.
When covid started last year, as someone young'ish and healthy I signed up to volunteer for human challenge trials and started to organize a convalescent plasma drive, because that's what I thought being civic minded meant. I have living family members who were affected by polio before widespread vaccinations were available, and recognize the importance of vaccines on herd immunity. After a year of hall of mirrors bullshit about masks and politics, I'm struggling with the case for why a low-risk healthy person would take a vaccine with non-trivial side effect risks for a virus that is less dangerous than their normal activities, when the vulnerable people who get vaccinated (for whom the risk/reward is clearer) are no longer vulnerable.
Is there a conversation to be had on the model for this, or does it come down to "conspiracy theorists who put us at risk," vs. "normal people" and there's no point in engaging it? Is the best argument just a matter of, "we live in a society and part of that is accepting the jab?"
Meanwhile we "anti-science" folks who have been blowing the whistle all along that the vaccines were not and could not even theoretically have been adequately tested (9 women can't make a baby in one month!) will just get shat on some more for some reason.
Because you will be held accountable for vaccination but not for progression of covid, you pull the lever to change tracks.
As one person draws it in Twitter: https://twitter.com/MiettinenTopi/status/1371702220174016520
Therefore, precautionary measures which respond dynamically to trends detected in newly available data, is the logical, ethical, and scientifically correct thing to do, imo.
I'm not saying the conclusion is incorrect, but it's driven by fear, uncertainty, and doubt -- not quite the same as a clear evidentiary basis.
That could be acceptable if the logic goes that AZN bears the burden of proving that every potential adverse side effect is extremely rare. However, by that logic the vaccinations will be paused several times and more people will suffer due to COVID.
https://www.nytimes.com/2021/02/08/health/immune-thrombocyto... (alternative link: https://archive.is/RisZF)
https://www.seattletimes.com/nation-world/doctors-death-afte...
We’ve had millions of doses in the UK without serious side effects, so unless there were faulty batches I think any risk must be minuscule, and certainly lower than the known risks of covid deaths for unvaccinated people.
This is a case where a cautious ‘first do no harm’ approach will likely cost many lives.
Also, I'm pretty sure each regulator knows the pros and cons of this decision, and they know well the consequences of stopping the vaccination - it's not like they are all incompetent. I mean, imagine the odds of the amount of ignorance to have reached this level of decision making in several independent countries.
Not likely, at all.
It's not a "a case where a cautious ‘first do no harm’ approach will likely cost many lives.", it's them doing their job and follow the procedure that has worked pretty well, based in science. It's what builds trust in vaccines and medicines, knowing that regulators are there, aware, and if they think something is wrong they won't take a stupid risk out of pride or pressure.
With this many countries pausing vaccinations, we know that there will potentially be thousands of extra deaths.
Google Translate: https://translate.google.com/translate?sl=no&tl=en&u=https:/...
> the benefits of the AstraZeneca vaccine in preventing COVID-19, with its associated risk of hospitalisation and death, outweigh the risks of side effects.
https://www.ema.europa.eu/en/news/emas-safety-committee-cont...
What's the thought process here?
EDIT: as pointed out elsewhere, the official press release gives us that there has been new data in the past few days with a specific concern, that's at least some info.
Is that guy wrong or basing the statement on outdated information?
WHO say no evidence of any risk https://www.bbc.co.uk/news/world-europe-56404542
I've personally seen the waiver forms send to doctors, and none of the usual testing was done, including the effect on youngsters, pregnant women, etc.
There is a very good reason we had these regulations in place to begin with.
tl'dr: Governments have let AZ off the hook legally if side-effects or worse occur.
I'm due to get vaccinated with AZ in less that two weeks and I will deninitely do it regardless, if doesn't get halted of course. Most EU countries decided to use it on recipients older than 55 and now they're halting it due to a baseless claim. It has worked fine and the UK has already vaccinated millions of people with it.
https://yougov.co.uk/topics/international/articles-reports/2...
The summary of the experts' opinion in the UK is that those countries' decision to suspend the vaccine is "baffling".
This has influenced public opinion in NL quite a bit ( in DE too I suspect ). I can read in the local comment sections that people want to decline the AZ vaccine as they don't trust it, and it is only 60% effective. They would rather have Pfizer, even Sputnik or rather no vacination at all than AZ. These commenters seem quite hostile to AZ and the UK for that matter.
And these comments are from before the clotting allegations.
This is and has been quite a contra-productive negotiation strategy from the EU commission, directly endangering public health in my humbe opinion.
> This is how a whole lot of people seek out happiness, by being "right" in their social circles, especially in a way that shows them as superior to large groups
And apparently they do this instinctively, without reflecting about it or understanding what they're doing (they do it also when it gives a silly impression, at least on me). It's hardwired in the brain I'd think
mikem170:
> Risk assessment isn't one of our stong suits, either
Long ago, in a hunter gatherer tribe, almost everything bad that you ever got to hear about, could happen to you too? So there was no need for the brain to get good at risk assessment -- just assuming that everything was "deadly dangerous" made sense, evolutionary?
Doesn't scale up well, with news from the whole planet
Some people are set to not take a vaccine, they will take whatever version of this story as an argument for their view point. It is not about them.
But take someone like my father (76) as example. Not anti—vaccine at all, but a bit cautious and not in a hurry to get it. If there are stories from reputable news papers, that vaccine A causes X issue but government keeps giving them out, he would not take it. If on the other hand it got stopped, investigated and found to be harmless he would be open again.
If based on the data it should be continued to be given out while investigation is ongoing, I don’t know. I think as with a lot of things about this pandemic and it’s handling in different countries it will maybe take years to have conclusive insights in hindsight what were the right decisions.
I don't think there's really a good answer here though. It's balancing human lives in the basis of imperfect data and predictions of human behavior.
When we’re talking about population-level inoculation, you need to maximize trust by minimizing any perceivable harm.
Should be investigated, and if it's a bad batch shouldn't be given to people.
Humans aren’t rational.
I don’t think that beurocrats are supposed to be leaders. The elected officials should be pushing for the change, not the people who run the operations.
Also the symptoms are bizarre, the deaths and hospitalizations from blod clot have all been young health care workers in good health with onset of symptoms a few days after getting their first shot. They have all had low platelet count which is very unusual with blood clots and complicates treatment immensely because the standard thrombolytic treatment is then not safe to use.
It's absolutely mad for Italy, Austria etc.
But this is not a surprise: countries that handle the pandemic well (evidence based rather than populism or dogma) continue to manage the vaccine rollout well, and vice versa.
But as more blood-clot deaths emerge... you gotta think caution is wise.
OTOH yes, we in the UK have administered a lot of this stuff, and you'd think someone would have noticed a serious side effect like this. So far reports from the UK seem to show no greater incidence of blood clot problems than would be expected without the vaccine.
Difficult to call, but I hope it's all being investigated thoroughly.
Important point! I start to get anxiety that there might be some Chernobyl level incompetence building up in our bureaucratic countries. I feel like we are getting to levels of a huge quantities of regulations, where then to unblock the process, relevant regulations are relaxed to be able to move forward, leaving us with a lot of regulations that make us feel safe, while the elephant in the room is building up through other valves. I fell like the 737 max thing also more or less fits this framework. So for the future: Let them incentives be aligned and them regulations work in the right direction!
We don't have time for that, we can't wait for some government panel to announce in 2025 "actually the blood clots were no more common than in the general population"
Last I saw it's 30 blood-clot deaths. Given the number of people that have received the vaccine that's a tiny, tiny amount. Even if those 30 were directly linkable to the vaccine (and so far no such link has been proven) you could still make the argument that the benefits of mass vaccinations outweigh the concern.
I don't envy anyone in charge of making those choices, though.
Apparently EU vaccines are produced in Europe, maybe there's something wrong in the local production facilities that's causing this. UK has only used AZ vaccines produced in the UK, afaik.
The equation changes when otherwise young and healthy individuals are at risk of serious complications, even if exceedingly rare.
> I don’t know anyone in pharmacovigilance who thinks what is happening now in EU states is rational based on known information.
> EMA had this right last week. We are seeing panic spread at EU state level.
https://twitter.com/isth/status/1370424157947752452
> The [International Society on Thrombosis and Haemostasis] recommends all eligible adults continue to receive the #COVID19 vaccine, despite recent decisions by some countries to at least temporarily suspend the use of the AstraZeneca vaccine due to reports of thrombosis. Read the full statement here: https://isth.org/news/556057
I would challenge the term "caution", as it implies giving the vaccine is more risky than not.
> Difficult to call, but I hope it's all being investigated thoroughly
I agree there. But rather not for medical reasons.
As far as I know by now a bunch of European countries have already suspended vaccination with the AstraZeneca vaccine. These include France, Germany, Italy and the Netherlands - not really a politically homogeneous bunch.
Litterally all members of the same economic and political Union. The EU.
Pfizer: https://assets.publishing.service.gov.uk/government/uploads/...
AstraZeneca: https://assets.publishing.service.gov.uk/government/uploads/...
Disclaimer from UK.gov:
Part of our monitoring role includes reviewing reports of suspected side effects. Any member of the public or health professional can submit suspected side effects through the Yellow Card scheme. The nature of Yellow Card reporting means that reported events are not always proven side effects. Some events may have happened anyway, regardless of vaccination. This is particularly the case when millions of people are vaccinated, and especially when most vaccines are being given to the most elderly people and people who have underlying illness. https://www.gov.uk/government/publications/coronavirus-covid...
Edit: Added disclaimer from UK.gov
Slightly different reporting periods but I'm pretty happy with the odds and I'd take either if offered.
I suspect it's probably "possible side effects and deaths within 28 days of administering a vaccine", in the same way that the UK records "deaths within 28 days of a positive COVID test". One does not imply the other was the cause. (edit) other commenter points to the official UK docs.
Even with that information, you need to know the non-vaccine incidence of the illnesses in that report to make any meaningful comparison and assessment of the efficacy of the vaccine. Which is what I rely on scientists to do.
From the horse's mouth:
Ann Taylor, Chief Medical Officer, said: “Around 17 million people in the EU and UK have now received our vaccine, and the number of cases of blood clots reported in this group is lower than the hundreds of cases that would be expected among the general population. The nature of the pandemic has led to increased attention in individual cases and we are going beyond the standard practices for safety monitoring of licensed medicines in reporting vaccine events, to ensure public safety.”
https://www.astrazeneca.com/media-centre/press-releases/2021...
The Yellow Card scheme and similar schemes are not useful for direct analysis, they're basically an aggregator for anecdotes. I had a mysterious craving for a kebab after the flu-like side effects from the Oxford vaccine subsided. Probably nothing. I'm not going to waste a doctor's time with a video appointment to report "I suddenly really wanted a kebab". But while musing about it I might as well fill out this web form (with the other boring side effects too), then it goes in the big pile and hey, maybe over the millions of shots given in this country they find 8000 people reported a craving for a kebab which is enough to be interesting even though it's unclear how that could happen or what you should do about it.
Medics are going to write a lot more of these. Patient comes in with unexplained back pain, can't recall any triggering incident, but they did get the Pfizer vaccine 10 days ago? It goes in a Yellow Card report. Again, probably nothing, patients turn up with unexplained back pain all the time, vaccine or not. But collecting these anecdotes gives us a better chance to spot real problems early, so long as we don't mistake them for serious data.
Can we please fucking stop the downvotes?
Imagine they went against this recommendation and it turns out there is indeed an issue with the vaccine. That would cause a shit storm of epic proportions. This way the "worst" that can happen is that there was a delay.
Now people could die during that delay because they weren't vaccinated, but it's much easier to sweep that under the rug as a politician, in my opinion.
If mostly old people die from COVID but the adverse reaction of the vaccine is independent of age, then for very young people the risk of an adverse reaction of the vaccination might outweigh the risk of permanent damage from COVID.
And not just because of the obviously higher risk associated, but also because it appears not to be effective against the new strains. (Especially the new South Africa strain). Unlike for example the Janssen vaccine (goes by their parent company of Johnson and Johnson in the US) which was actually validated in South Africa or the rna ones which are just a technical masterpiece.
Keep in mind that the real shortage of vaccines is production locations right now. And the type of production of the Janssen, AZ and the Sputnik vaccine is all similar. So why even produce more of the worst vaccine in any of these locations.
BTW I literally just had the Astra Zenica vaccine here in UK - I have a sore arm, lets hope I don't get any of the reported side effects!
Make sure to get plenty of water and rest :)
Germany has high rates of vaccine hesitancy. One way to tackle that is to be extra cautious. So, as soon as there's information about problems the vaccination programme is halted, an investigation is carried out, accurate and clear information is then presented showing rates of harm in unvaccinated and vaccinated people, and the programme is restarted.
Just a thought with zero data behind it...
Twitter thread with some commentary & sources:
The Irish reasoning for suspending AZ wasn't just because of blood clots but blood clots in the brain which have a completley different severity.
https://www.astrazeneca.com/media-centre/press-releases/2021...
https://www.theverge.com/2021/3/7/22318113/russia-intelligen...
When you plot the infection and death rates of the vaccinated vs the unvaccinated population, the rates in the vaccinated group drop like a stone. The effect is highly significant.
The vaccination strategy is highly effective and is absolutely a major contributor (if not the primary contributor) to the decline.
'See, we were right not to vaccinate this fast'
For the downvoters: https://www.theguardian.com/commentisfree/2021/mar/15/eviden...
Am I missing something, how's that supposed to help ?
The alternative Pzifer jab is 10-20 times as expensive.
That is a lot money, some of which may find its way to work the media and the decision makers.
https://www.ft.com/content/c474f9e1-8807-4e57-9c79-6f4af145b...
AstraZeneca vaccine document shows limit of no-profit pledge
Company has right under contract to declare pandemic over by July 2021
- Johnson & Johnson (USA)
- Sputnik V (Russland)
- CanSino (China)
You can't make the same decisions about risks when you have one side so skewed by age. There is absolutely no guarantee that side effects from vaccination would be a preferable risk for younger populations or that vaccination side effects would have comparable age-related effects.
Covid response isn't a religion, it's not "we have to do everything" or "we shouldn't do anything", responses need reason not gut reactions.
Depending on the type of adverse reaction, it might be safer for young people to not get vaccinated at all or with a different vaccine. (For example if the adverse reaction affects mostly young people, while COVID affects mostly older people.)
I believe it's likely that lockdowns may cause some deaths, or possibly even lots of deaths. However, they certainly help prevent the spread of deadly disease too and hence prevent many deaths. We can probably get fairly definite numbers on how many deaths lockdown prevents in a large population. I don't think we can get similar numbers on how many they cause. My gut says they probably prevent a lot more than they cause, but I'd like to see any studies on this, if anyone has a link to share.
I feel bad for people in countries where people are even restricted from being outdoors, despite hearing again and again that outdoors is the safest place to be.
Do not forget that these vaccines are still very new, plus there's the possibility of a production issue with the AZ vaccine that affects only part of the production; I wouldn't say it's "politically-motivated" or a dumb idea to pause AZ vaccinations until one does a deeper investigation; I personally chose to avoid AZ due to a history of strokes in my family, I preferred to reserve a spot on the Moderna list. Better safe than sorry.
There's a lot of good reasons for choosing a vaccine even if the risk isn't strictly zero. And you also need to remember that receiving vaccination isn't mandatory. If you personally aren't comfortable with the risks you don't have to get vaccinated.
This makes me skeptical of the suspension, but I'm not an export on these matters and haven't done enough research to claim to have done my due diligence, so I'll refrain from either advocating for or against this step.
So they are only technically allowed to adjust the price to take into account the different operational costs depending on the manufacturing site.
[1] https://www.fiercepharma.com/pharma/astrazeneca-puts-a-time-...
I do think people aren’t giving AZ enough credit for doing it at cost though. Especially compared to the €50 per dose Pfizer initially quoted the EU!
The UK and EU supply chains are completely separate to the best of my knowledge. The UK manufactures and packages its supply, and the EU manufactures and packages its supply.
I read an unsourced claim on HN a few weeks ago that they did 9 phase-3 trials, and applied for approval on the basis of only 2. Which would be rather bad if true. Moreover, it is clear that their 1.5 dose regimen was a mistake in trial execution.
Meanwhile, the FDA still hasn't approved AZ.
It seems possible that AZ was overeager to present good results, and thus was less cautious than they should have been. It's only a possibility, but its one that worries me.
Anyone here have an source to confirm / debunk the rumor that AZ did 9 trials, and only applied on the basis of 2 trials?
edit: I just looked at the stats in the UK, and it certainly seems like since they started vaccinating cases have dropped off, and deaths have dropped of even faster. Since vaccines are probably targeted at the more vulnerable, it certainly seems to show that the vaccine has very positive net effects.
EU is buying vaccines with profit margins, and those are delivering.
If that cost structure is proving to not be enough for AZ, then they shouldn't have accepted it, because clearly what they are doing now is borderline criminal, all while hiding behind a "best effort" clause in a contract, that's being stretched far beyond what is acceptable.
They messed up the trials, they set up production infrastructure that would have never worked to begin with (because of the UK contract not allowing exports of vaccines), giving notice of failed deliveries on short notice, and still make new promises of deliveries that are showing yet again not to be true. They are yet to file approval for other production facilities in EU that should have been working for MONTHS.
Now they dare to question independent regulators from different countries by saying their vaccines are fine - when they didn't seem to even have bothered to investigate any of the cases - it's like they looked at a spreadsheet and said "this anomaly is within these intervals", completely disregarding the type of cases, their local incidence, time window and age group. Ignoring the fact that these occurrences are 4x greater then the ones in the UK.
I understand that the EU doesn't want to file a lawsuit because it's counter productive, but at this point I think it's the only path - pull the funding, place it on other candidates, sue AZ. It's too much incompetence for such an endeavor, which makes you question if they are not simply cutting corners. Again, they seem to be pushing "best effort" to what is acceptable.
https://mobile.twitter.com/politicsforali/status/13714790084...
My very rough calculation: There are ~ 200,000 vaccines administered daily in Germany, of which maybe 50% are AstraZeneca, so lets say we are delaying 100,000 vaccines / day - corresponding to 0.1% of the population vaccinated with Astra-Zeneca per day. Currently there are ~ 200 daily COVID-19 deaths in Germany, so in proportion one would expect ~ 0.2 additional deaths per day (~2 per week) due to the delay.
Assuming people prioritised to get AstraZeneca are 10x as likely to die from COVID than the general population, this still leaves us with 20 deaths / week due to the delay.
The big question is now how many people will die because they are infected by someone who could have gotten vaccinated sooner, but with a R of ~1, and less than 20 weeks until the whole population is vaccined, I doubt this will give two more orders of magnitude.
the usual figure now is 5 Million vaccinations and 30 reported deaths from blood clotting. Which appears to be not much different from the number without vaccinations.
https://www.nbcnews.com/news/world/oxford-astrazeneca-vaccin...
Until of course it's yourself, a family member, or a friend that joins the rank of those 300.
You're criticizing EU commission for transparently expose the shortcomings of this private company, but you seem to forget what this wave of what apparently are thousands of "internet specialists" that know better then independent regulator bodies for medicines.
Yes, this isn't EMA (that British propaganda painted as a slow and incompetent agency) - it's each country own regulator that have been responsible for the safety of millions of citizens, and they have been doing a pretty good job for many, many years.
This isn't a joint operation. It's scientists expressing their concern about these cases which are anything but normal.
Or now, every single EU country regulator (including Norway) are all incompetent, including the doctors who reported these cases and are following closely their development? They're all in this conspiracy to put down AZ?
I mean people rightfully criticize anti-vaxxers, but trust me, this bullshit attitude is just the same as the anti-vaxxers. It's blind fanaticism towards a vaccine, that even science should be disregarded, exactly the extreme opposite of anti-vaxxes.
AZ was considered less trustworthy than Pfizer or Moderna vaccines several months before that due to irregularities in phase 3 clinical trials (original dosage leads to ~62% efficacy, while inadvertently given half-dose to a part of test subject leads to higher efficacy): https://www.thelancet.com/journals/lancet/article/PIIS0140-6...
Conflicts between AZ and EU commission seems silly compared to that and IMHO lead more to discreditation of Ursula von der Leyen.
source? Yes, there is some negative opinion about this, but at least in Germany it's much more based on media citing "government sources" and general FUD tactics than anything the commission has said.
> accumulation of a special form of very rare cerebral vein thrombosis (sinus vein thrombosis) in connection with a deficiency of blood platelets (thrombocytopenia) and bleeding in temporal proximity to vaccinations with the COVID-19 vaccine AstraZeneca.
Perhaps really just a bad batch somehow if this particular complication wasn't observed in the UK.
[1] https://www.pei.de/EN/newsroom/hp-news/2021/210315-pei-infor...
It's hard to say if this is a good decision, my impression is that this is too risk-averse given the real danger and very significant chance of COVID 19 infections. But it does seem to be based on different data than just a few days ago.
PEI Statement:
https://www.pei.de/EN/newsroom/hp-news/2021/210315-pei-infor...
Anyway, here's the UK's disclaimer from the Yellow Card summary link you posted.
Part of our monitoring role includes reviewing reports of suspected side effects. Any member of the public or health professional can submit suspected side effects through the Yellow Card scheme. The nature of Yellow Card reporting means that reported events are not always proven side effects. Some events may have happened anyway, regardless of vaccination. This is particularly the case when millions of people are vaccinated, and especially when most vaccines are being given to the most elderly people and people who have underlying illness.
We who? If you're talking about healthcare the chances of survival are constantly moderated by various policies ( both government and private ) against the money spent.
It kind of feels like people are only now reading the note that comes with a drug. And we are using these drugs on millions of people, so yeah even the one in a million complications will start to show.
It sure seems that AZ is singled out on that so. And I really wonder why. Because it sure is getting into dangerous territory by now that we are artificialy limiting our vaccine availability.
Of course this is an exaggeration, but there is a somewhat disturbing neglect of EU elections, functions and political appointments in the public view (it's seen as less prestigious than national/federal elections in many EU member states).
As a result, it's a climate that doesn't always attract and get the leadership it really needs (given that the EU formally and practically overrules legislation and jurisdiction of member states).
My point still stands: with vaccines, you can’t create reasons for distrust.
Does aspirine not cross the blood brain barrier?
But it doesn't mean that you will surely get COVID if you refuse to get a shot. Also, some people claim the vaccines are not very effective against some variants such as the South African one. So it means you can get vaccinated, suffer some serious side effects, and once you are recovered, get COVID.
As opposed to who? I see tons of scientists proclaim things as ‘proven’ which later turn out not so true after all.
I suppose it depends on the alternative - if it's "not having the vaccine" clearly that's worse. If it's "controlling the death rate by prolonging lockdowns" then that's clearly not desirable either, but not quite as bad.
If it's just "give a different vaccine", then that would be no problem. Of course then there are the supply issues it's unlikely that simple.
The majority of people getting the vaccinations are older. Perhaps we will see more cases will emerge for the younger age groups.
Regarding the strains, all vaccines are less effective against the South African one.
Maybe they won't let you know, to avoid people refusing to get the AZ "vaccine".
How long until you can buy it? This way it's not a (possibly corrupt) politician deciding which corporation will make the stuff that gets into your body.
They are hopefully scientific, but they are definitely not independent, not even by name.
Usually I don't read notes coming with meds, but I am almost sure that even everyday stuff has potentially deadly side effects in the ball park number of the blood cloths AZ is causing.
Yes, some drugs have pretty nasty side effects, but vaccines are rather special, because their acceptance affects the entire society and vaccine safety is a sensitive topic, especially in a climate of skepticism. Undermining the idea of vaccine safety will be much worse than Covid (at least at this time).
And there would probably be an investigation into that the moment people using them showed up growing a third arm instead of getting a trombose.
From personal experience today (spouse getting second dose of Moderna), the nurse explicitly suggested using Tylenol to handle fever in case it occurs.
Here is a quote from https://www.cdc.gov/vaccines/covid-19/info-by-product/clinic...:
Management of post-COVID-19-vaccination symptoms
For all currently authorized COVID-19 vaccines, antipyretic or analgesic medications (e.g., acetaminophen, non-steroidal anti-inflammatory drugs) can be taken for the treatment of post-vaccination local or systemic symptoms, if medically appropriate. <ellipsis>
I'm not worried about blunted immune response because I've taken heaps of asprin when I had COVID-19 (it might be why I got tinnitus for close to 6 months afterwards -- that or the antibiotics) and I mean grams per day and I had very high antibodies levels afterwards.
(Not a doctor) From listening to the "Faucis" of various countries (incuding the original): I believe that the vaccine is not a watered down virus, so technically you are not making yourself vulnerable/more sensitive to the virus. It is suppsed to 'teach' your body how to build the defence.
Only the Chinese virus is a 'watered down' version of the virus. All the others (including the Russian) is an RNA-type-thingie.
No where did I say any of these vaccines are 'live' or even attenuated coronavirus. It is 100% impossible to get infected with covid-19 from any of the vaccines. However it is possible to take a drug which lowers your immune system response and you fail to build a strong response to the vaccine and the spike protein RNA or other bits in the vaccine. Hence why I said _talk to your doctor before doing anything like taking aspirin right before the vaccine_.
This site is full of pure lunacy when it comes to any COVID-19 or medical issues. The comments in this thread and many others over the past weeks are just unbelievable low quality. Folks, stay in your lanes with software and startups...
"If the rash is itchy, you can take an antihistamine. If it is painful, you can take a pain medication like acetaminophen or a non-steroidal anti-inflammatory drug (NSAID)."
No need for speculation. RTFM applies here, too.
https://www.cdc.gov/coronavirus/2019-ncov/vaccines/safety/al...
This is not true. There are 11 current vaccines in use around the world, of 4 different types. Even the vaccine mentioned in this article is an adenovirus-vector vaccine.
The Pfizer-BioNTech and Moderna vaccines are the only mRNA vaccines.
https://en.wikipedia.org/wiki/COVID-19_vaccine#Vaccine_types
I hope it's being invested thoroughly by the people that know this stuff inside out, from AZ, Oxford and doctors on the ground where this has happened
Damn right a government panel is useless here!
Germany for example has nearly 2 million doses they are delaying, so that's ~300 deaths per day that are caused by these delays. If you delay by a fortnight that's more deaths than on 9/11.
That being said a lot of Europeans who would come to the UK would be appalled by the quality of NHS compared to other European countries.
So I would argue that I would trust what German NHS says more than the British one.
People (especially on HN) like to say "correlation doesn't equal causation", but there isn't even a correlation here. There are not higher rates of blood clots.
The majority of the vocal deniers is localized around Munich btw, same with homeopathy advocates. Not sure why that is but I suspect 1888's medicine book by Eduard Bilz, which was extremely popular in Germany, could play a role (https://de.wikipedia.org/wiki/Bilz-Buch).
It's going to be interesting to see if western europe doubles down on the anti-vax beliefs or they swing round to be more like the Ossis.
[1] has a chart showing the percentage of kids born in 2012 getting full measles vaccination within their first two years by county.
[1] https://www.sueddeutsche.de/bayern/oberbayern-murnau-hauptst...
(I’m looking at the linked PDF https://www.pei.de/SharedDocs/Downloads/EN/newsroom-en/hp-ne...)
https://www.worldometers.info/coronavirus/coronavirus-death-...
The 0.0015% is the known rate of blood clots from all the AZ doses on the continent according to what the GP has reported and RFI has confirmed the same numbers today (30 cases in 5M doses but it's not clear how many have died and why).
So 0.4 death rate times 0.004 chance to get covid in my area equals 0.0016 chanches to get covid and die which is one point higher than the chances of getting blood clots from the vaccine. Yeah, I botched the last product, so it's actually about the same risk figure, but the benefits of getting vaccinated outweigh the risks and the allegedly faulty vaccine batch has already been halted anyway. I have acquaintances that were vaccinated with the allgedly faulty batch AVB2856 before it was halted and they're doing just fine.
The 0.0015 risk of death seems high. Where are you getting that from?
https://www.reuters.com/article/us-health-coronavirus-german... gives "The EMA has said that as of March 10, a total of 30 cases of blood clotting had been reported among close to 5 million people vaccinated with the AstraZeneca shot in the European Economic Area, which links 30 European countries."
But if you want to take the German numbers, 3 deaths out of 1.6m vaccines:
3/1,600,000 = 0.000001875 (In percent, 0.0001875%) which is 0.125 of your figure.
And the OP gives a base rate of "two to five cases per 1 million individuals per year" for context; we need to subtract out the base rate from the observed deaths too (because obviously the base rate of this condition occurs regardless of whether you take the vaccine).
[edit: percent conversion typo]
It is (or was), AZ was to supply EU with 500M vaccines this year but changed that to 200M.
EU got really served on the vaccine front, UK got more from AZ, US got more from Pfizer/Moderna (both have 3x more vaccinated than EU). And each transport that we ought to get is smaller or dalayed.
I wouldn't be surprised if governments there blocked some of the vaccine export.
I really hope that there will be a backslash for those companies for not fulfilling their obligations. If not now then later when there is a race for subsidies for "free" prescription medications.
The best strategy (however cynical) is to not be quantitatively explicit about expectations so that you can frame it as though you succeeded no matter what happens.
What if that turns out to be more difficult than you originally realized.
It is 0.58% of all deaths being caused by covid. As in 994 out of 1000 people under 18 died in the same period from other things.
Compared to people who are alive covid killed 0.000288% (or 1 in 350,000) under 18s.
30 in 17M is too few to have a reliable statistic, but that comes out to 1 in 567,000.
If that holds, is age invariant, etc. etc. and ignoring the time-based nature of the covid deaths, taking that vaccine would represent a *50%* increase in death risk for under 18s, which is just absurdly high. (it doesn't matter that that 50% isn't exactly right, anything remotely close is an unacceptable risk)
Statistics is hard.
Since everyone is expected to get the vaccine, it's not fair to compare COVID deaths / total deaths to vaccine deaths / total population, you need to compare COVID deaths / total population to vaccine deaths / total population.
In this case, assuming the numbers posted are remotely accurate, then this specific vaccine could end up being far more dangerous to people under 18 years of age compared to getting COVID and waiting it out for two weeks.
We don't know and I'm not asserting one way or another. I'm just saying that making comparisons is much more difficult and nuanced than the straightforward naiive approach.
(I'm not commenting on how to solve this equation, just pointing out other factors)
If the covid risk was flat over time, if you offered this vaccine yearly (quite possibly necessary) then you'd be saving ~90 lives in this age bracket per year. 10 would still die of covid, 100 would die from the vaccine, 90 whom would have died of covid would would instead survive.
It would be "better" depending on how you think about better. Telling people to throw away huge chunks of their lives to protect against a risk that you turn around and tell them they need to take a risky vaccine that's only half as bad... it isn't necessarily a good line. Especially because pandemic diseases tend to lower in their negative outcomes at time goes on, the vaccine will probably stay the same while the risk it prevents will get less and less threatening.
All of this based on statistics and assumptions that have a lot of uncertainty in them.
The bottom line is that in order to be a good idea, a vaccine needs to be much safer than the disease it prevents. Half as risky doesn't meet this mark; AZ would be fine for the oldest age bracket because the risk profile wouldn't change much, but the youngest age bracket there is a significant comparison between the two (and perhaps further unknown risks which haven't surfaced)
> AstraZeneca on Friday said unspecified export restrictions now rendered plans to bring in large amounts of doses made outside Europe unlikely.
This suggests that countries outside the EU have imposed export restrictions that contribute to the vaccine shortage.
I assume this is referring to the US export ban. It definitely isn't referring to Italy.
All of this over the 3.8 million doses they bought, and were intercepted and taken by Italy (whose export control already reduced the shipment size to 780k doses).
This would explain why the Swedish state were so heavily criticised for not locking down. Also would explain the UK government arresting people for being outdoors (there's not really any data supporting outdoor transmission, that I know of).
I haven't had any luck with that. I assume these numbers are what the FDA is looking at. Possible side effects are documented in the packaging for a drug, but that doesn't qualify the risk without numbers. I'd prefer to know this for any drug I'd consider using. I find it strange that this data is so hard to find.
I ask because it sounds like you went pretty deep in the vaccine you mentioned, maybe you bumped into this.
I have no idea what OP means when he says “following it closely” as that’s impossible beyond press releases.
There is definetly a couple of case studies for a lot of discipline in that. Besides virology, epidemiology or medcine.
To be fair, AstraZeneca wanted to ship those to Canada and Mexico, but Biden (and earlier Trump) has forbidden exporting vaccines out of US.
Also weekly report of the covid-19 vaccine side effects here: https://www.gov.uk/government/publications/coronavirus-covid...
Had my jab 3 hours ago, and enjoying a nice honey dew pomelo as I type thinking, fruit just don't get any better than this.
First it was efficiany with elderly in the study, were the numbers were totally misunderstood. Then it was overall effectiveness, then prevention of severe cases. The list goes on. In the meanwhile, the press is reporting every single rash people get with AZ.
EDIT: Just checked, they found 7 cases of thrombosis in the brain, out of 1.6 million vaccinated people. Well, we'll see how that develops.
I don't think they are trying to get revenge. They are trying to cover for their own failings. By any reasonable means, the vaccine rollout in continental Europe in relation to the wealth and logistics available compared to US/UK is a complete failure.
Except, you know, order enough vaccines for their population. Other than that though, everything that they can!
And yes, governments are doing everything they can. And the screw up with vaccinations. No idea why, because I don't have all the details, but maybe AZ is just coming in time to have been 1) a good scape goat early on when one was needed during the frustration with vaccine deliveries 2) bad at PR 3) earned a bad rep and now everybody is over cautious. And public / media pressure isn't really helping.
The base rate is per year, the AZ vaccine was used for about 3 mo in the EU. That leaves us with a base rate of 0.5 to 1.25 cases per million per 3 mo, so using your numbers:
1.875 - (0.5…1.25) = 1±0.375
deaths per million if we were to keep the inputs unchanged?
https://colab.research.google.com/drive/1C7K3u3vKrIMt-sa4_t3...
The first cell is the model I was building, I finally got it into reasonable shape. It comes from the published national statistics for death rates. (Comments welcome, I just sketched this to help me think about the numbers here. No claim on this actually being right.)
The second cell is my attempt at rendering your initial calc, though I've not folded in the base rate changes. We can go into the weeds there but looking at the results I don't think we need to; my calcs naively attribute all the blood clot cases to the vaccine and still give COVID as being worse than the vaccinations by a factor of 400-800.
The way you're thinking about base rates sounds right to me though, and it does sound like the best guess is we're at something like 4x above base rate.
Given that I implemented my model with a completely different approach and we're both within a factor of 2 (if I've rendered yours correctly) I think we're in the right ballpark here, at least for "Fermi calculation" level of completeness.
Guardian article with more numbers: https://www.theguardian.com/world/2021/mar/16/benefits-of-as...
Neither of us was doing that so far. Case mortality seems to be the best basis, adjusted maybe for overall risk of infection when everything is opened up and nobody is using masks anymore. At which point any comparison most likely degenerated into guess work.
The main difference so is that vaccinations reduce the overall risk for the population. And we didn't even talk about severe long term effects of COVID.
That being said, we live with a lot of medications that have severe side effects in the 1/100,000 plus bracket without breaking a sweat.
By the way, I don't see how you come to the conclusion that the AZ vaccine is in any way riskier than COVID.
The challenge with COVID as always is that the risk of death is correlated across the population. So a 25 yo having COVID increases the odds that he dies and that everyone around him dies. But that’s a whole other discussion.
Isn't that the case? At least in my country, there is no obligation to take the vaccine, and even incentives (e.g. being able to attend public events sooner) are seen very critically.
For my age cohort the chance of death from either is infinitesimal but because of Bayes it might make sense to continue to avoid both, but if I try to explain that to my peers they might think I'm a Trump supporter, and as everyone knows, Trump supporters should be shunned from polite society (especially since the "insurrection"), so I see this as a choice between social excommunication and a questionable injection I don't want
Fun times
To me, these vaccines have been as rigorously tested as they could be, and none of this was really ever about people in your health category anyways, so that seems irrelevant in the “utility of vaccination” argument.
I could be incorrect though, so I’m interested in your unease and rejection of what I find to be sound science.
More importantly it’s not just about avoiding death, a bad case of COVID is terrible even if you survive. On top of this you reduce the risk of spreading it to someone else.
That doesn't work so great if you don't die and have lifelong complications, though. It doesn't work so great if you get it and kill your child/grandmother either.
It doesn't work so well if you have to catch the virus multiple times to have immunity either (folks aren't always immune after catching it). Not to mention the unknowns with mutations of the virus.
It is seriously much better to try to avoid catching the virus at all. The virus means you might be ok... or you might die, or you might have a lifetime of suffering that you wouldn't get with a vaccine.
https://qcovid.org/Calculation
eg. 30 year old healthy white male: 1 in 7,092 risk of hospitalisation, 1 in 250,000 risk of death.
By contrast the risk of death from anything for a 30 year old male in the UK is 1 in 1,215:
http://www.bandolier.org.uk/booth/Risk/dyingage.html
Even taking a healthy 80 year old male, the risk of death from COVID is 1 in 275, whereas the annual risk of death from anything is 1 in 15.
But it's not just about the risk to the individual. It's about the risk to the population as a whole. Both of these risks need to be balanced.
While the vaccine might not /appear/ to be worth it at a young age, by getting vaccinated and blocking the transmission of the virus you are protecting the population at large. From that perspective, not getting vaccinated is actually very selfish (using the exact meaning of the word).
People need to look at both the personal and societal aspects of the vaccination strategy. There will be social pressure to be vaccinated because it's not just about you, it's about everyone, and if we are to reopen society and get back to normal, then the expectation is that nearly all of us will need to get vaccinated.
- Death is not the only bad outcome. Many otherwise healthy younger people have experienced months of debilitating sickness, in addition to weeks of the worst flu you've ever had.
- You can pass it on to people less fortunate than yourself, who can't take weeks off work, and (in some countries) may not have health insurance, and might be at higher risk of death or morbidity.
- You're burdening a stretched health system, literally preventing other people (or even yourself) from getting life saving treatment.
- You're stopping me and everyone else from going to the pub.
The vaccine greatly reduces the chances that I have any of these things. Or heck, it even greatly reduces the chance that I'll have a week or two of misery.
The fact that we have insufficiently tested vaccines does make the decision harder.
The most sensible thing is to investigate this, maybe more without the vaccine died from thrombosis, but need to see.
Pull the lever, and the lever might do things you didn't expect - like derail the last few cars. Don't pull the lever, and people die for sure.
If you derail the last car and don't try to put it back before the next train, you now suddenly have more folks that don't trust the lever and avoid all trains, not just the one you operate.
There must be no doubts with vaccines, 100% trust in them is essential.
Completely unrealistic. Everything in life has associated risks, and vaccines do carry a (small) risk.
It would be better to educate people about understanding and balancing relative risks rather than sensationalising a few outliers. The main fault here lies with the lack of proper rational discussion in the media.
people are such cool "lever pullers" until that one person is themselves.
It's pretty obvious there's a profound psychological, developmental (children), and economic toll of lockdowns.
For anyone that's below 60 or so, it's very clear they've got net negative effects on their life from draconian across the board measures that go on this long.
edit: wow immediately flagged? Is it verboten to mention the simple fact of economic trade-offs in any decision we make?
I'm not even saying that lockdowns are bad, I'm saying that they have profound consequences that can't be brushed away or ignored.
The fact that so many are reticent to even admit that is why I think it's so important to mention it.
For a source https://www.google.com/amp/s/mobile.reuters.com/article/amp/...
I don’t attempt to extend that to more developed countries however. And I can’t say they things wouldn’t be worse if they hadn’t locked down, but according to a family I know in Uganda, they were locked down before they had even one case. I haven’t done the research on whether that is true or not so take it or leave it.
"In summary, we fail to find strong evidence supporting a role for more restrictive NPIs in the control of COVID in early 2020. We do not question the role of all public health interventions, or of coordinated communications about the epidemic, but we fail to find an additional benefit of stay-at-home orders and business closures.
The data cannot fully exclude the possibility of some benefits. However, even if they exist, these benefits may not match the numerous harms of these aggressive measures. More targeted public health interventions that more effectively reduce transmissions may be important for future epidemic control without the harms of highly restrictive measures."
[1] https://pubpeer.com/publications/3D81CAC483C2021C00E27C8826D...
I don't know how you know that. Given the significant time and effort required to become a doctor, isn't it at least as likely that they are motivated about people not dying on any lawn?
A handful of unjust police killings cause widespread protest / riot / unrest, but 15,000 unprevented homicides are largely accepted as part of life.
You can argue that they are morally equivalent, but our brains get more angry at someone doing a bad thing than at someone not doing a good thing.
Most of the public doesn't care or understand, neither do the politicians. Not interesting to fix because no one intentionally did anything bad? And, spending time on this won't win any elections?
What about the Hippocratic oath? First do no harm.
https://covid19criticalcare.com/medical-evidence/methylpredn...
Still, the consequences for those unfortunate riders can stay with them throughout life.
Ride safe.
From an article titled "Lab studies suggest Pfizer, Moderna vaccines can protect against coronavirus variant" I quote:
"While the blood serum samples produced less neutralizing antibody activity, it was still enough to neutralize the virus, they wrote in a letter to the journal. This is in line with other studies. And it's well within what is seen with other viruses, one of the researchers said." [1]
[0] https://www.google.com/search?q=covid+immunity+from+other+co...
[1] https://www.cnn.com/2021/02/17/health/pfizer-vaccine-south-a...
The problem however is those with weak immune systems. In these cases, the vaccine is unlikely to help these people much, and they become breeding grounds for escape variants.
It's like taking a quarter dose of an antibiotic, against an infection of an organism that tends to mutate at a high rate. This places a large pressure on the organism for an escape variant.
This is exactly what Bossche warns of. Listen to minute 37 onward: https://www.brighteon.com/257797f0-06fa-4596-be69-af71bb3adc...
Goals and announcements have already been missed, and it turning out to be unnecessary can be muddied, or buried.
Assuming this is indeed politics, there are a lot of positives to this type of move in an already shit situation.
Are we still having this debate.... Of course the overall mortality didn't change much, people stayed at home for literally 75% of the year.
Do you have the split stats for accidental deaths, road deaths, disease related deaths, &c. ? Because otherwise it's meaningless. We can put everyone in an artificial coma and get as little death per year as possible, it isn't a really interesting metric without the context.
It shows that despite everything we've done we've had significant more deaths in certain age groups.
You seem to be genuinely curious. For those who want to scoff it off: look at those numbers and consider the fact that these numbers are what we see after a war-sized effort to prevent more damage: in most populations only a few percent have been hit.
At the moment this epidemic runs unchecked a death rates also increase even more as it easily overwhelms even European health care if it isn't kept down.
And no, it is not just the elderly: my age group (40+) and above are all at risk.
Which doesn't seem to have worked - infection rates are dropping off all around the world, regardless of the vaccination levels. It looks more like we hit natural herd immunity at about the same time in different places whether or not masks and lockdowns were used.
Sweden, 2020 deaths only 6.2% higher than 2018, and following a weak 2019 flu season.
These are entirely acceptable death figures within the context of aging European societies.
COVID is basically a once-a-decade flu variant: like Swine Flu in 2009, which came and went without lockdown: https://swprs.org/wp-content/uploads/2020/10/sweden-monthly-...
So COVID is dangerous enough to lock down entire societies, but not dangerous enough to justify continued vaccination when 1 in 166,666 have blood clotting? This is probably the background rate.
It seems like Europe and its bureaucrats just can't let go of lockdown. Or alternatively, they wish to push the vaccines and end of lockdown into Spring/Summer, where natural seasonality will take care of COVID and give the appearance that lockdown and vaccines were a success.
https://brnodaily.com/2020/12/16/news/excess-mortality-rate-...
And that's old numbers, since then the situation only got worse: https://www.aljazeera.com/news/2021/3/15/czech-republic-what... https://edition.cnn.com/2021/02/28/europe/czech-republic-cor...
Did you somehow forget that this is the second year of Covid? We've already gone through the whole "natural seasonality" cycle and the disease is very much still here.
(In reality, in Sweden mortality is about 4.5 % higher than the average of 2015-2019, but that is still very significant; and of course, covid is not just that one either dies or is fine; there is the substantial but currently not very well known number of people with long-term health impact from the infection)
It's not about the "oh it's worth the risk compared to COVID 19". If it's a side effect it wasn't spotted in the trials, why was that?
It's not a side effect? It was a problem in production? What problem? Was is tampered with or was an accident? What failed in QA to let that batch come to the public? Was is a storage problem that compromised the batch quality? Was it while in transport or in the local hospital?
You talk about this like background noise. It's not. It should be investigated.
It's good that this is happening, because it shows regulators are doing their job. This is what builds trust in vaccines, not disregarding odd occurrences because they seem to have no "statistical relevance". That's just ignorance talking.
Imagine this is the outcome of a production problem, yet regulators refused to acknowledge this until it was out of proportions because the problem wasn't fixed. Not only people would lose trust on vaccines, they would lose trust on the regulator - this extends far beyond this vaccine, but all vaccines and medicines.
People need to feel safe, and to know that regulators are not sleeping on their job. It's not a bureaucratic job, but that they are actively looking at data and reports from doctors.
It's not a political decision no matter how many people try to spin this. This is the outcome of doctors reporting an anomaly to a regulator. The system is working, and this should give you reassurance, not doubt about the consequences of stopping a vaccine.
I'm pretty sure they know the consequences of this setback, so for them to stop it it's because something is not right.
This is not established at all.
Overall the number of blood clots observed is actually less than expected, with an incidence lower than in the general population (i.e. without vaccine at all). My source is BBC News this evening.
>To me, these vaccines have been as rigorously tested as they could be
Not for me. The fact is, the vaccines have been pushed through faster than any vaccine before. Anything foreign entering the body should be tested and based on solid evidence. Doesn't matter if it's an artificial heart, stent, prosthetic, or a biological agent like a vaccine. If decades of medical research shows determining a vaccine's safety takes years because of ethical protocols, then it takes years. The present vaccination campaigns are performing more comprehensive stage 3 trials on the general population because the risks are deemed acceptable. As other people have said in this thread, a person under the age of 18 is 50% more likely to die of SARS-CoV-2 vaccine complications than from SARS-CoV-2. The risk isn't worth it at this time.
Additionally, the technologies being used for the vaccines is still deemed experimental, specifically the mRNA ones. No mRNA vaccines have been deployed before, but now it's being deployed on the general population without public knowledge of any potential risks of this unproven technology ("unproven" meaning lacking a prior real-world deployment effort; a rocket engine is only proven when it flies, not in simulation). One risk with the mRNA vaccines is that they need to be kept extremely cold to preserve the mRNA sequences [1]. If the dose warms, good mRNA sequences break down into junk mRNA, which for all intents and purposes are random nucleotide chains. That ties into an above point: no rational person wants random mRNA pieces put into their body. Again, while all risk is relative, for my age group, the risk is not enough.
If you're well-versed in the science, I recommend reading this complaint [2] filed with the EU regarding Pfizer trial safety.
[1] https://www.reuters.com/article/uk-fact-check-mrna-vaccine-s...
[2] https://2020news.de/wp-content/uploads/2020/12/Wodarg_Yeadon...
This pandemic was never about the risk to this cohort that continues to be brought up. The point is that taking the vaccines reduces deaths. In places where these vaccines have been deployed widely, you cannot refute that statement. Just because the people who are dying don’t look like you does not diminish the utility of the vaccine.
I’m so tired of hearing that young people shouldn’t take the risk of vaccines because the risk to them of the virus is less. That is not why anyone at all is urging you to get the vaccine, or why we did any of this at all for a year.
A society is built on mutual trust and actions and speech like this shatter it; the selfish arguments seem to know no bounds in this pandemic. I did not sit in my damned house for a year because I was afraid for my own safety!
Furthermore, The article linked claims PCR testing isn’t good enough for efficacy and from what I understood had nothing to do with safety at all. In fact, the title of that submission includes “... REGARDING CONFIRMATION OF EFFICACY” and no mention of safety, but maybe I’m not “well-versed in science” enough to understand it. Thank you for talking down to me though, we would not want me to leave this conversation with a sense of self worth.
It seems to me like you’re unintentionally spreading disinformation. I assume you don’t want to be doing that, so you should probably check your priors here, as they seem to be outdated.
I watched enough of the video you sent to see what Dr. Bosche was saying - that vaccination immunity is more specific than natural immunity, and that may present problems down the road with variants. I also found this note/presentation/slides by him [0]. I read some of this to get more detail, video is kind of lame for relating so much information. I'm not a virologist. But I have read a bunch of this stuff. I thought what Dr. Bosche said was interesting. I had a few initial questions. I'd love to see more virologist's opinions on this.
He says "Covid-19, a highly mutable virus, only needs to add another few mutations in its receptor-binding domain". I didn't know that covid19 was considered highly mutable, like the flu. Is he hedging here, saying this might happen? I guess the specific proteins that the vaccines target would need to mutate. I wonder how likely this is. I assume there are lots of things that are "several mutations" away from killing us all. Papers I've seen early on said that left to its own covid19 had a 50/50 chance of mutating to become no more deaadly than the common cold (because it would spread better that way), or settle into something that flares up every few years, like a bad flu season. I took that to mean that there are also pressures to mutate to something less deadly. They think this is what may have happened in 1873 (if memory serves), a new coronavirus came on the scene, it looked like a very bad flu season at the time.
He mentioned several cases of young people dying from covid19 variants, and several cases of people shedding variants. "Several" is not a large number, especially considering how much we don't understand about the immune system. Typhoid Mary was shedding for years, and that had nothing to do with a vaccine. I don't know that I'd consider his several examples to be anything out of the ordinary out of a sample size of how many tens of millions.
He seems to be saying we'd be better off if we didn't proceed with vaccinations and allowed the population to reach natural herd immunity at this point, since covid19 has already spread to so many people. That people who caught it and got better on their own would be better protected. This reminds me of the virologist early on who recommended finding the least deadly variant and spreading that around on purpose.
It's an interesting topic, and I appreciate you bringing it up! I don't mean to argue over it, so much as relay my thoughts and left some of the details of what he's saying.
Do you think most of the people fearful of variants are on the same page with this guy? The news stories I see mentioning problems with vaccines and variants don't ever seem to have solid sources/studies backing them up, I've never heard this guy mentioned before, and he seems to be a relatively lone voice at this point. I'd like to think that the experts have had a chance to hash all this out amongst themselves, but I know things don't always work out that nicely.
[0] https://www.deblauwetijger.com/wp-content/uploads/2021/03/Ge...
Source: https://opencovid-peru.com/reportes/sinadef/ (1100 deaths per day, compared to 300 average for 2019)
At the beginning of the pandemic, it was believed that the virus was using droplet transmission alone. In such a scenario, surgical masks, for the general public, would only be required in people who were sick to prevent transmission and N95 masks would primarily be required by health care workers. Considering the mask shortages faced in many countries at the time due to panic buying, the communications made by governments to the public w.r.t the benefits of masks make sense from a cost benefit perspective since it would guarantee that the people who needed the masks the most (medical workers and sick people) would receive them and reduce the spread of the virus.
Fast forward 2 months later, airborne transmission as well as asymptomatic transmission of the virus were both confirmed independently in several labs. This would mean that the prior strategy of only using surgical masks on sick people wouldn't really work well anymore. In the meanwhile, the availability of masks was much higher due to increased production. Hence, to reduce the risks of airborne and asymptomatic transmissions, governments released advisories asking all people to wear masks.
When officials start doing this, you have to play a sort of game where you try to figure out why they said something and what it signifies. You have to try to divine the state of reality and figure out what to do based on what you think they were trying to get people to do (there's a lot of uncertainty in this).
By that point, by definition, trust in the person (and probably the institution) is gone, and we don't have a lot of trust in institutions to spare.
Now anti-maskers and other covid deniers are citing that report: "don't do anything, even the government research says it is useless".
But of course if a government official lies to you about your own health risks then that has very high costs, much higher than whatever masks were saved. They could have just said "masks are useful, but you need to be trained to use them correctly, they are difficult to manipulate, etc. and they are very scarce so sadly let's stay home and let doctors and nurses use them".
I might sound as if I'm upset at that, because I REALLY am. I hate when governments lie, even if they are "white lies", and I hate when they treat their constituents as kids.
As a citizen, would you trust the government if they did yet another 180, after demonstrating to you 2x that they didn't actually know what they were talking about?
One of the many things that I've learned from this pandemic is that for better or worse, the answer to this question is emphatically yes for a significant percentage of the population. Many folks will indeed blindly trust whatever they are currently being told by people they believe are authorities or experts. At times this may be a good thing, but I personally lean toward thinking it's not good overall. And as you correctly point out, another big chunk of people will understandably lose faith in institutions and authorities that either were wrong or simply lied, which I'd argue likely causes significant long term damage to the healthy functioning of a society.
> Considering the mask shortages faced in many countries at the time due to panic buying, the communications made by governments to the public w.r.t the benefits of masks make sense from a cost benefit perspective since it would guarantee that the people who needed the masks the most (medical workers and sick people) would receive them and reduce the spread of the virus.
The government lying to its people is never acceptable. Also, there was plenty of time to ramp up mask production when the virus was spreading in China and later Italy. Taiwan did this successfully, why did supposedly more developed countries fail so badly at ensuring adequate mask supply?
People never look at "date of death" or "infection date" all they care about is "reporting date" - and every newspaper out there will show you the effects of government measures on "reporting".
Wow, this is exactly how the masks thing played out in Poland. I wasn't aware that this "makes are useless" followed by "masks are mandatory" (with Poland together with a ban on selling them on the biggest platform, big like Amazon is in the US - Allegro).
And now here in Poland we are at the "AstraZeneca vaccine is safe" and we are vaccinating with it, I wonder how many EU countries still use it besides Poland.
https://en.wikipedia.org/wiki/Parallel_trading_in_Hong_Kong
Globalization came to bite the hand that easily gave production out of hand for single-use items.
I mean some people were looting pharmacies for chloroquine so lying at that point on masks is almost a security issue..
Risks of long-term consequences don't seem to be all that low.
A year ago there was a lot of noise about things like heart issues induced by COVID, which turned out to be mostly statistical errors in the papers that made the claims.
A lot of people (often people who never actually had a positive test) also claim to suffer from various mental impairments after their COVID infections, and some newspaper ran an article saying that some of these symptoms were alleviated after the people were given anxiety medication. Go figure ...
Check out this: https://www.biorxiv.org/content/10.1101/2021.02.23.432474v1
The Spanish Flu has led to a „sleeping sickness“ epidemic years after it ceased.
I’ll let the eventual studies give the percentages. But my (personal, non professional) take on this is that long-hauler experiences are a LOT more common then people realize, have been fairly ignored while people have fixated on the death count, and have big possible implications for quality of life for younger, otherwise healthy people.
Long covid:
> Estimates of the number of people with long COVID vary widely. In July, the US Centers for Disease Control and Prevention reported that one in five patients 18–34 years of age without chronic medical conditions and with a positive outpatient test had not fully recovered by 2–3 weeks after testing, and a research center in Rome found that 87% of 143 patients reported persistence of at least one symptom 60 days after onset of the disease. According to a preprint published in October that has not yet undergone peer review, 24% of 233 patients still had symptoms at 90 days after infection. Data from a smartphone app, as reported by the COVID Symptom Study, showed that one in ten patients with COVID-19 have symptoms after 3 weeks. Given the scale of the pandemic, if even only a small percentage of the tens of millions of infected people worldwide develop long COVID, a staggeringly large number of people would need long-term follow-up and treatment.
"Paediatricians in Israel, which has surged ahead in vaccinating its adult population, reported a sharp rise in covid-19 infections among young people, with more than 50 000 children and teens testing positive in January—more than Israel saw in any month during the first and second waves."
A single metric (e.g. positive tests) is not enough to assess any severity here, and even those metrics come with caveats because all of our methods of determining them are imprecise.
https://www.economist.com/graphic-detail/covid-pandemic-mort...
>Or let people have a choice in determining whether the risk is worth it for them.
Are there any countries where the vaccine is mandatory? That choice already exists doesn't it?
On the other hand, getting a potentially faulty vaccine would seem to mostly only be a risk to the individual, although I suppose there is some risk of overwhelming hospitals still.
Please just stay home for a few more months so this shit can finally fucking end. It’s already been a year.
Edit: an important factor, too, is that understanding the potential risks of the AZ vaccine is hard, and the average person may not expected to fully understand them. Right now, it seems like even the authorities don’t understand them.
(Edit: Deleted second paragraph that wasn’t clearly worded.)
Covid is transmitted mostly during its mild phase, it only becomes severe a week later, if you are unlucky. If you are lucky, you clear off the infection and gain relatively strong immunity. For the virus, both scenarios are similar.
The only thing is that if it was just a cold, we wouldn't bother with preventive measures and the virus would spread more easily. However, when both the lethal and nonlethal variants are present, the nonlethal variant doesn't have an advantage since we treat everyone the same way, so it is unlikely for the nonlethal variant to take over on its own. At least not on a short timescale.
The solution is to create our own nonlethal variant, also known as a vaccine. Well, vaccines don't spread, I guess we could make a vaccine that spreads but "what could possibly go wrong..."
The virus needs the host in order to spread. The virus doesn't have any other ulterior mechanism that wants to kill humans.
This is why spanish-flu virus got weaker over time because as it evolves, if it kills humans rapidly, it cannot evolve. So, nature sorts it self out.
Banning everyone from getting this vaccine is typical bureaucratic ass-covering. Their incentives are not aligned with ours. They get in trouble if they’re directly responsible for a few deaths, but not if they’re indirectly responsible for hundreds of thousands of deaths.
To give a point of comparison: 250 miles of driving gives you a one in a million chance of death. This vaccine is safer than that.
It's not bureaucratic ass-covering, it's literally the protocol that's in place and has worked to keep populations safe.
>250 miles of driving gives you a one in a million chance of death. This vaccine is safer than that.
Again you're missing the point. The correct analogy would be: driving on a car that randomly combusts, or has faulty breaks, due to bad QA. And this actually happens/happened, that's why some cars are pulled from the market to be fixed when such things happen. Doesn't matter if it has happened on 1 or 2 cars, it shouldn't happen. Want another analogy?
Want another example? The Boing 737 Max.
You should only be allowed to use products that are working as expected, not faulty products. Specially not medicines and vaccines, that could blow up the trust on regulators and the vaccines.
There is no safe option here. We have to think like we are in war time, not peace time. Allowing people with informed consent to take this vaccine will save far more lives than banning everyone from taking it.
Yes, then it starts to have an impact; without those, there would have been mayhem.
For the two additional things you've mentioned: Limiting travel works to prevent the virus from entering an area, but if it's already there and uncontrolled it wouldn't have an effect. Likewise excessive hand disinfectant doesn't seem to have had an effect, because the virus doesn't really spread through surfaces like that [0] - it was an early precaution that wasn't reexamined.
With that in mind, and knowing that these were only two of the many measures made to reduce the infection rate, your parahprased statement "the measures were meaningless because they didn't stop the epidemic" is completely incorrect.
An epidemic isn't on or off. It develops at different rates, exponential->logistic if R>1 and exponentially dampening if R<1 for each area. A very steep exponential phase will obviously cause the problems we have been trying to avoid, and it's similarly obvious that the defensive measures have prevented that outcome most places.
Germany provides a useful testbed for the impact of mask usage, because the mask mandates have been decided on local regional levels (federal state or city) at different times. From these different times of mask mandates and different progression of epidemic in the areas that are otherwise comparable, we can see that mask usage has a clear impact.
As said, it doesn't stop the epidemic alone, but it helps to contain it. To beat it, we need immunity through vaccines.
It did work, hospitals can only absorbs so many patients in ICU per weeks/months. Once an hospital is at 100% capacity people start dying because they can't be treated (not only for covid)
It really isn't rocket science, of course natural herd immunity is helping, spreading it over a year vs a month is a game changer though.
> Moreover, the database is not a representative sample of the sars-cov-2-positive population. Because it only contains records from people who have interacted with a medical service provider, it excludes those who weather the disease at home without medical assistance.
This will exclude the vast majority of people in younger age groups who were affected. Serology studies have shown us that in many densely populated places infection rates have been far into the double-digit percentages - if this statistic was true in the way you interpreted it, we would know that by now.
But in Germany and Europe children can't get vaccinated and by the time young adults can it will be September anyway.
http://www.iayork.com/MysteryRays/2007/08/26/rabbits-1-virus...
"It's not a political decision"
From the perspective of the regulators, there are asymmetric personal consequences.
If they make a decision that leads to 50 clotting deaths but saves 5000 people from COVID as a counterfactual, their head is on a chopping block because those 5000 foregone deaths are invisible but the 50 deaths are visible.
If they make a decision to halt the vaccine distribution and this kills an extra 5000 people - well that's no problem because they were just being careful.
Society has set up a political situation where there is literally only one choice that absolves the bureaucrats from a negative personal outcome. Of course they're going to go that route.
Personal incentives are incredibly powerful drivers of behavior, whatever the publicly stated reasons for an action may happen to be.
It may be the case that they've made the right decision, but we can't assume that it was for the right reasons.
I'm more saying that the incentives of regulators/politicians aren't always aligned with public health, since the decision that protects public health and the decision that protects careers aren't always the same thing.
But what are “the right reasons”? This one is a moral dilemma that has no solution. “OK, let’s kill these 50 people so that that those 5000 could live.” No one in their right mind can propose that.
Well that's arguable, I haven't had covid yet, and I don't plan on getting it. You had plenty of countries that handled covid without vaccines - we are where we are because western governments refused to take specific measures to control de pandemic (but this is another subject). So the alternative would be get a different vaccine.
Neither me EMA, or any regulator are advocating for not being vaccinated, I don't get where you're getting that from. The alternative to this vaccine is other vaccines, in EU alone 4 vaccines are approved and more are to come. Even AZ vaccine isn't excluded what so ever - they are investigating the potential cause.
>Allowing people with informed consent to take this vaccine will save far more lives than banning everyone from taking it.
Thankfully we have regulators that prevent such behavior. If there's a QA issue no one should be vaccinated with the batches affected by that, because proper QA seem to be without any of this reactions.
https://covid.cdc.gov/covid-data-tracker/#trends_dailytrends...
From an average of about 50k cases reported daily in April through October to about 200k cases reported daily in November, December, and January, then back down to 60k by March.
And there's a similar winter increase in the worldwide cases (some of which is from the US cases, but not all):
https://www.worldometers.info/coronavirus/worldwide-graphs/#...
It's impossible to be sure after just one year, but that hill in the winter certainly suggests a seasonal illness to me.
Further, South American countries were some of the worst hit during the Nov - Feb timeline. South Africa was badly hit around this time. And all these are Southern Hemisphere countries that were experiencing summer around then.
Now, there’s clear evidence that warmer weather makes things easier, since the virus has lower survivability outside a host in the heat, so all things equal, the spread would be lower in warmer weather, but it’s not so much lower that it can be considered seasonal, like the flu.
Same reason it was rampant in the US subtropical south during last summer, when it was uncomfortably hot and people stayed inside where there's AC.
They're referring more to, success can be claimed for lockdowns/etc whether or not they had an effect, simply by waiting until the natural seasonality causes a drop in cases.
I'm saying that looking at aggregate outcomes and comparing locations that took these precautions to ones that didn't, this isn't obvious at all. It looks to me more like these defensive measures didn't work, and I kinda want to know why, if they're as effective as the percentages you gave.
It's hard to find a society that took no measures, as the measures so obviously work and no one wants an uncontrolled epidemic, but there's plenty of societies that had differing degrees of catastrophe up to the point where they realized this or started being serious about it. Czech Republic, Peru, Brazil, Bergamo (the latter just being unaware) +++.
Covid initially had a reproductive number between 3 and 6 in the absence of measures - higher for the latest mutations. A cumulative reduction of R of 80% + 40% would make this an R of ~0.25-0.50, but that's assuming 100% compliance everywhere and always.
Indeed, this is what you see in societies that were serious enough but didn't eradicate the virus altogether -- largely no significant epidemic, but wildfire-like eruptions of disease in local communities that don't strictly follow the measures. E.g. classrooms, public transport, homes, pubs/concerts and so on. Norway, as a case in point, currently has an R of 1.33, with measures that kept R cleanly below zero until the British mutation became dominant (through initial seeding through import and then a few almost-inevitable cases). Cities where measures can almost always be followed have almost no disease, the illness only spreads in areas where many people live close together and have children/teenagers in school. This alone is enough to threaten the capacity of intensive care.
Personally I don't really think this merits much debate anymore, if the objective is to seek the truth rather than some ulterior motive (e.g. politicians who wouldn't mind if the pension liabilities fell). It's not subtle if you actually dig into the details.
> Since encephalitis lethargica’s (EL) prevalence in the 1920s, epidemiological and clinical debate has persisted over whether EL was caused by, potentiated by, or merely coincident with the Spanish influenza pandemic. Epidemiologic analyses generally suggest that the disorders were coincidental.
https://en.m.wikipedia.org/wiki/Encephalitis_lethargica https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2778472/
https://www.cdc.gov/coronavirus/2019-ncov/long-term-effects....
I like to believe that these institutions - regulators - know better then to cover their asses, because if that was protocol until now for sure there would be a lot of problems with medicines and vaccines.
At leas the European ones (the cases I know) seem to have been pretty competent on their jobs, so I doubt that is a motivation.
I'm not sure what your point is with the apparent difficulty of understanding the risks of a new vaccine. Are you saying "it's hard, so just trust what the authorities tell you"?
To be clear, we’re talking about the risk of the AZ vaccine specifically. It seems like there might be something specifically wrong with it. Ceding approval authority to bodies like the FDA is how medicine is regulated all over the world. That’s how literal snake oil is blocked from sale. Among other things, it prevents desperate patients from making uninformed, dangerous, and expensive treatment decisions. The average person really isn’t equipped to read a medical study and adequately interpret the results. This information isn’t even at the maturity level of a study, and the risk is that people hurt themselves and undermine the confidence in this vaccine and others.
As for your comments on regulation - yes, that is correct, which is why I was surprised when I got so much flak for pointing out that, at least in the UK, regulatory shortcuts were taken to rush the approval of Covid vaccines.
FWIW, the LCD of most relevant studies show that maybe banning large gatherings is useful, whereas all other measures we've invented in the meantime have dubious efficacy at best - and extremely high costs.
There are plenty of places in the world that didn't implement the "fight COVID at any cost" policies and they're doing just fine. Trust me on that, I live in one of them.
> where natural seasonality will take care of COVID
I don't read that as your interpretation at all. It very much sounds like they are saying the spring/summer season will kill COVID.
There were shortcuts taken in all countries to get the vaccines out. In the US, there is no FDA approved COVID vaccine. Every “approved” vaccine is actually under an emergency use authorization.
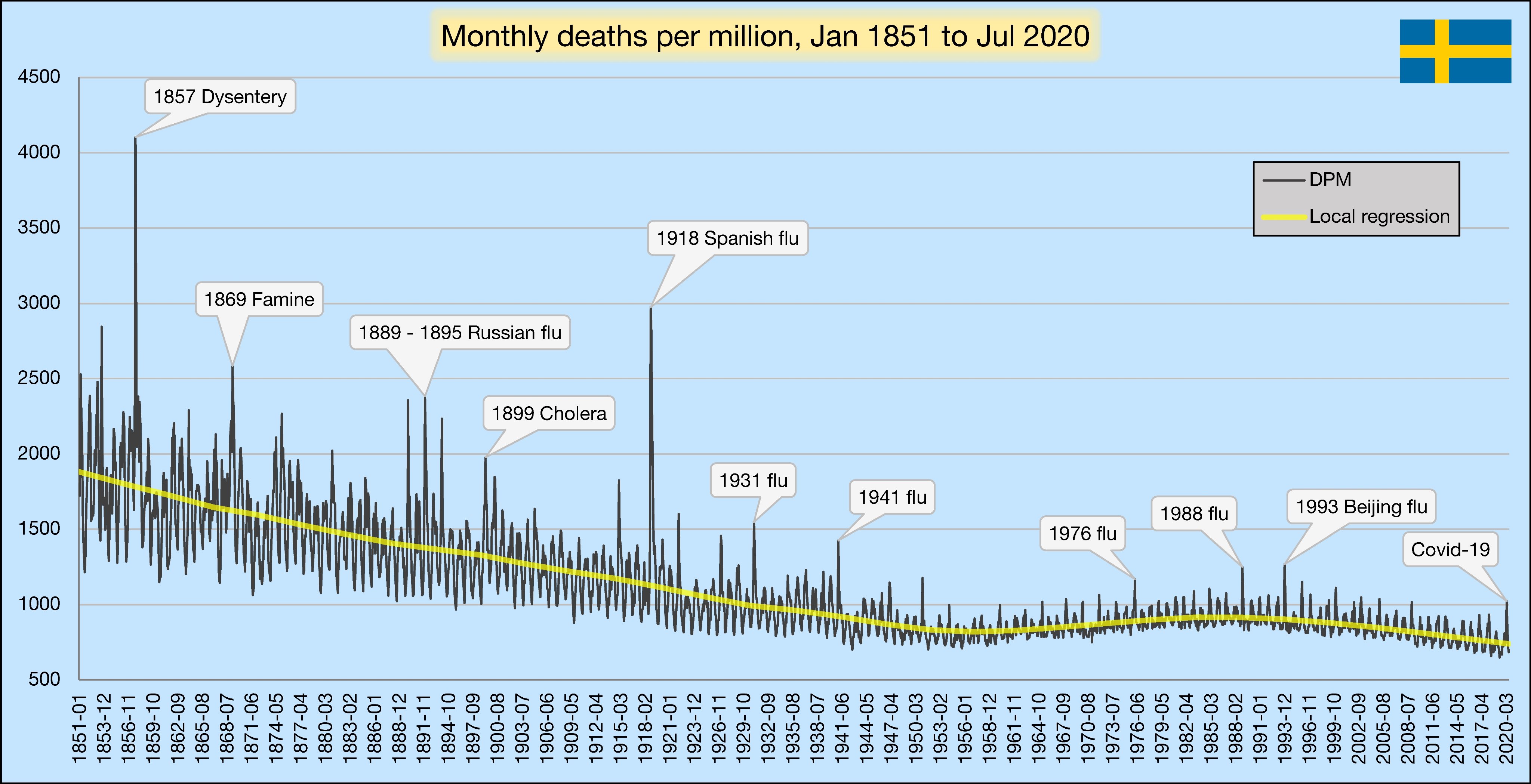{kind=link}