In case you hadn't heard, the Cleveland Clinic--consistently regarded as one of the top hospital systems in the United States and in the world--recently shared a study of 52,238 patients showing zero incremental benefit from the jab to the previously infected, recommending that "people who’ve had COVID-19 don’t need to get vaccinated."[2]
[1]https://www.nature.com/articles/d41586-021-01442-9
[2]https://www.healthline.com/health-news/new-study-determines-...
This study ended May 15, 2021, and it notes that:
>Lastly, it is necessary to emphasize that these findings are based on the prevailing assortment of virus variants in the community during the study. It is not known how well these results will hold if or when some of the newer variants of concern become prominent.
Another study found that, for people already seropositive for SARS-CoV-2 antibodies from a previous infection, getting the first dose of an mRNA vaccine increased antibody titers by two orders of magnitude on average [1] but that the 2nd dose had no effect on antibody titers.
[1] Florian Krammer, et al. "Antibody responses in seropositive persons after a single dose of SARS-CoV-2 mRNA vaccine." New England Journal of Medicine (2021). https://www.nejm.org/doi/full/10.1056/NEJMc2101667
That's not what this says -- you're extrapolating that the vaccine somehow changed the immune response, when this letter is only providing data that people who already had Covid had a clear, ~immediate antibody response to vaccination. That's exactly what you expect to happen when immune people see an antigen for a second time.
In other words, the previously infected recipients already had a well-primed immune response. The vaccination isn't necessarily doing anything to increase the response -- it's just the expected reaction of an already-primed immune system, when it a bolus of antigens it already knows about is injected into the body:
> The antibody titers of vaccinees with preexisting immunity were 10 to 45 times as high as those of vaccinees without preexisting immunity at the same time points after the first vaccine dose (e.g., 25 times as high at 13 to 16 days) and also exceeded the median antibody titers measured in participants without preexisting immunity after the second vaccine dose by more than a factor of 6.
If anything, this letter (not a paper) provides further evidence that vaccination for the previously infected is not necessary.
"Individuals who have had SARS-CoV-2 infection are unlikely to benefit from COVID-19 vaccination, and vaccines can be safely prioritized to those who have not been infected before."
And from the body of the article:
"Experts say that more research is needed to determine how long immunity lasts after a case of COVID-19. Until we have that data, some infectious disease specialists are recommending that people who’ve had COVID-19 still get one dose."
And:
"Given the limited availability of the vaccines in certain countries, the findings add to the growing belief that the vaccines should be prioritized for those who haven’t previously had COVID-19."
Is 12 to 15 weeks (3-4 months) really "long lasting" antibody mediated immunity? I'm glad the antibodies still neutralize even gamma that long but 3-4 months is the timespan people were previously calling "short". Yes, T cell responses (the cells that kill infected cells) to sars-cov-2 epitopes last longer (not covered in this article) but this just seems to confirm the short coverage of b cell mediated antibodies.
It's perfectly normal for an antibody response to decay over time. We don't keep making antibodies in perpetuity for every antigen we've ever seen, or our blood would turn into peanut butter.
The B-cell and T-cell mediated responses to previous infection are also proving to be robust, and the B-cell response, in particular, primes the immune system for a rapid increase in antibody levels if the virus is encountered again.
Reinfection studies from a few months ago demonstrated that natural immunity is roughly 50% effective for people aged 65 or over. And that's the age group most likely to experience negative outcomes from covid-19, it's seems prudent to go ahead and recommend vaccinations for this age group, regardless of previous infection.
Then there's the elephant in the room: so few people have been tested that it really difficult to know who has had it. Anyone who has had a cold in the past 18 months is going to claim they had covid, regardless of whether they tested positive or not. It would be easier to vaccinate this group than it would be to perform a test for covid antibodies.
If covid hadn't become a political shit-show, I'd agree with you. But at this point, I think it's a little irresponsible to society to give anyone an out on getting vaccinated.
We have evidence that vaccination continue to provide broad-spectrum immunity while those naturally immune are e.g. still vulnerable to the Delta variant [1].
[1] https://directorsblog.nih.gov/2021/06/22/how-immunity-genera...
Also, generally speaking, people who caught COVID were contagious for a while, while vaccinated people aren't. So there's the social responsibility factor - if you have a lifestyle where you at all likely to be among people while contagious, getting vaccinated reduces risk for others.
Really, "naturally immune" would imply a pre-existing immunity to the infection.
https://www.bbc.co.uk/news/health-57640550
> “people who’ve had COVID-19 don’t need to get vaccinated.”
Having had Covid twice myself (different variants?), I don’t agree!
Resistance to SARS-CoV1 has lasted more than a decade. Coronaviruses mutates far less dramatically than influenza does.
Especially among young adults teenagers and children since they have yet to be vaccinated at scale.
Edit to add: 70% effective vs. 95%+ is a significant reduction.
Does the delta variant and others pose the same risks? Are we over responding to a virus family group?
> My understanding is variants of highly dangerous viruses rarely keep the high level of risk as the progenitors.
Even if that's a general trend that doesn't mean it's a rule. And the rationale "a dead host isn't as useful at spreading the virus" doesn't really apply to covid since only a small percentage gets hospitalized or dies, most infectees remain fit enough to spread it further.
Moreover, Pfizer is partner of BioNTech, which developed the vaccine. I don’t understand why OP omits that and solely credits Pfizer.
Pfizer is easier to type than "Pfizer BioNTech" (there's 3 capital letters in that second word, 2 next to each other).
Laziness wins.
Edit: I should say I'm expecting to see that it was not impactful. Would still be nice to see papers on it.
They seem “unreasonably effective” against COVID, basically if you had a genie that you could ask to make a vaccine, it would be hard to do much better, other than the requirement for 2 jabs.
In addition, the mRNA technology has broad applicability to other issues such as other viruses (such as flu) and even cancer!
The US has moved past isolation, its just not going to happen again, there is no political will for it. I fully support vaccination, I just don't support a police state asking to check our papers.
Seems clear we can, and do, forbid individuals from physically and financially harming the community by their ‘personal’ choices. It is their body and their right to do as they wish — perhaps only as long as it harms no others who have the right to be unharmed.
What problem does a domestic vaccine passport solve?
The same problem the Yellow Card [1] solves. Right now, I have a New York State electronic passport and a CDC paper proof of vaccination. The former works in New York City. The latter works across the U.S., at least now. (At least, it worked in San Francisco and Atlanta.) If I travel abroad, I may need to get the latter re-certified since it's trivial to forge and not independently verifiable. Having a single, authoritative document fixes all this and makes socializing and commerce more frictionless.
If we don't want to go into another lockdown when the Delta variant hits, we need to be able to isolate the vaccinated from the vulnerable. The former can continue mixing and mingling with reduced (though not zero) risk of causing a flare-up. The latter, I don't know, ideally they'd stay home but we know that won't happen.
What does that mean? Vaccination is not a political position in most other countries - it's just a policy goal at a national level.
The goal would be to give local governments and businesses an approved way to understand who has received the vaccine so they could open up safely.
A centralized database that is used to control individuals is akin to China's social credit system. I've actually started seeing people argue for China style systems, and I find it both frightening and sickening.
When I start to push back at all, I usually get arguments like `Leave the US if you don't like it.`, and sure I'll just pick up and leave the country I was born in, but beyond that where will I be able to go?
If I just want my own individual rights, where in the world will I be able to go if what is basically the last bastion of freedom and individualism is lost to tyrannical majority rule?
+: Let's be honest, driver's licenses are practically required and you attract extra scrutiny if you don't have one.
To be not aware of this on place like HackerNews is... not very believable, we discuss this all the time, every day.
"last bastion of freedom" - there are places like Switzerland which have more of freedom than any place in US. There is no power nor amount of the money in the world that would force me to move from here to police state like US where everybody talks about freedom but only top 0.1% enjoys some of it.
This might be hard to grasp, but it should be generally true also in US - your freedom ends where other's begins (ie transportation, coming to any work/office). With Covid, this is valid 1000x more. Freedom and anarchy are not the same as some hardliners would like to believe.
https://en.wikipedia.org/wiki/International_Certificate_of_V...
Moreover, one of the first international certificate issued (1944) targetted Smallpox vaccinations and it's proliferation coincided with the booming air travel in the 1960's and 1970's. It is argued that the certificate was substantial towards preventing Smallpox from spreading in an age where endemic regions became only a few hours of flying away.
https://en.wikipedia.org/wiki/International_Sanitary_Convent... https://en.wikipedia.org/wiki/International_Sanitary_Convent...
The United States signed and ratified the Convention back in 1945, essentially acknowledging that countries are able to require U.S. citizens to have a vaccine certificate.
While the Convention dates back 75 years, today's Yellow Card is the de facto standard for certifying that you have gotten shots at a border.
COVID-19 poses a challenge as this disease is highly infectious and crippling enough that preventing spread has become a far bigger global priority then other infectious diseases such as Yellow Fever. However, as of yet, a digital, secure, widely adopted solution that goes beyond the WHO's Yellow Card is still in the works. Several airlines and the IATA are working on their own travellers pass, but realistically, a trusted vaccination passport which is globally recognized requires an international treaty between nations governments. The world hasn't arrived at this point yet, and most countries still operate their own systems such as passenger locator forms or national passes issued to their own citizens.
https://en.wikipedia.org/wiki/Vaccination_requirements_for_i...
https://www.reuters.com/business/healthcare-pharmaceuticals/...
(I legitimately don't know and I am curious. I see the article does reference protection against a variant during a study, but it's unclear to me if that means all future variants as well.)
The reason we won't need yearly vaccinations as with the flu shots isn't a property of the mRNA vaccine, it's a property of COVID-19. The watered-down explanation is that this particular sort of virus simply doesn't mutate as much as the flu virus because it has a mechanism that prevents it. We do see variants, but they're actually quite similar so the same vaccine still works (thankfully).
It's also why we're talking about COVID "variants" and flu "strains". In this context, a different "strain" usually signifies different surface proteins, i.e., you need a different vaccine for it. I don't believe that we've seen a second COVID strain yet.
My guess would be that commenter doesn't provide any evidence to support his/her claim. (I didn't downvote it, BTW.)
https://www.cnbc.com/2021/04/15/pfizer-ceo-says-third-covid-...
https://www.cnbc.com/2021/06/22/covid-booster-shots-coronavi...
The news of this new study just came out today. Give the guy a break.
AFAIK not really. I know just about Sinovac and that was significantly worse efficacy than other vaccines. Note that adonovirusvector based vaccines like AstraZeneca one are not 'traditional vaccines' but also rather new tech.
Just like with mRNA; viral vector vaccines haven't been seen widespread use before COVID either. And the only attempts at an attenuated vaccine have been pretty ineffective as far as I know.
[1]: https://www.canada.ca/en/public-health/services/immunization...
"Follow up earlier post. Here is moderna/pfizer/wild type spike. There is only 2 amino acids different from wild to vaccine. Same for both vaccines. The change forces the protein to look like it would when stuck to the outside of the virus, without needing the rest of the virus"
From Thought Emporium on twitter (cool biohacker with particular focus on genetic engineering, but amazing breadth into physical sciences as well - I highly recommend his youtube channel)
https://twitter.com/EmporiumThought/status/14081777241920675...
[1]: https://www.medrxiv.org/content/10.1101/2021.05.22.21257658v...
should we see a variant that escapes this RBD Antibody mechanism then there will be a possibility of escape, and concommitant requirement to tweak the vaccine antigen.
If you're talking Alpha vs Delta and about hospitalisation/death, then the vaccines are actually marginally more effective against Delta than Alpha according to data from Public Health England (although there's significant overlap in the confidence intervals).
Software engineers (engineers in general actually) aren't special at all when it comes to being rational. They just like to think they are because of their field. It's identical to Stephen Hawking thinking he had special insight on politics, because he was gifted at one thing; or a famous actor thinking they have special insight on politics because they're gifted at one thing. Engineers are just as prone to failing to control their emotions properly, bouts of subject irrationalism and failing to strive for objectivity as is the typical person. Your typical software engineer on HN is no more rational than the typical plumber, the plumber is just likely more honest about it and less full of their self. You see it in every thread on HN, yet the rational engineer myth persists, amusingly.
Yellow card is for some international travel and school enrollment. It is not a vaccine passport, so while I appreciate engaging the question, it's not clear that this is the same use case. Nobody asks an adult for their measles vaccination status in a normal domestic interaction like a concert, train, office, etc.
I think most people should get vaccinated and we can all move on with our lives, however, I also think a generalized vaccine passport for domestic use is an abomination with inevitable and horrific consequences, and so I am trying to get a sense of what the sincere case for it is. If it's just leveraging the crisis to institute bureaucratic social controls, I'll be the most reasonable man on the barricades.
We need a better "why" that is actually true, and not a cynical "noble lie," (like masks/no-masks was), because when you actually get off the internet and talk to people, it's the percieved lies and the attitudes of the people who tell them that are creating the hesitancy.
If a covid-unvaccinated person goes into a stadium or bar full of covid-vaccinated people, what is the effect? The only way the shots get more traction is with a clear and honest answer to that, imo.
Check https://impfdashboard.de for up-to-date numbers.
Much of the data comparing efficacy of 1 vs 2 doses doesn't wait until 10-days after the first dose, which defeats the point. That being said 2 doses is more effective, just not by as much as you'd might think.
edit: replaced the above link because it was pay-walled
> There are tons of central databases you are already registered in, all available on demand.
Most of these are not ran by the government though. Thus their use is not mandated.
> your freedom ends where other's begins
In libertarian circles this is generally spoken about as the `non-aggression principle`.
I in no way think that a proof of vaccination system put together by private providers, coupled with businesses' choice to check vaccination status is wrong. I do think the responsible thing to do is somewhere along the lines of self isolating to either being vaccinated or having an antibody test.
My objection is a government orchestrated vaccination database with mandated use in private businesses.
edit: I don't know why you're being downvoted, but I did upvote you for the thoughtful commentary. : )
In Arizona, it's required that all immunizations given to <=18s are reported (along with "encouragement" for providers to report adult immunizations) and this is the basis for determining if the child may attend a public school, for example.
Generally agree, but have fun finding a place to live though, it seems around me even small landlords seem to want credit checks.
(Genuine question.)
If you're a vaccine maker, it's a good idea to have something ready if it turns out that a booster is needed. If you're in charge of public health, it's a good idea to plan for that possibility. That doesn't make it the plan yet.
Also note that you're looking at a press release. Scientific press releases take the information from the article, summarize it by giving the main achievement, removing any caveats, and otherwise presenting it in the best possible light possible. There are press releases like that for vaccines that were later shown to be ineffective, because at that point they were promising.
https://www.yalemedicine.org/news/covid-19-vaccine-compariso...
I'm not saying that out of skepticism for these vaccines, I think it's amazing we're deploying all these new platforms. I just think saying that they're no more effective than vaccines we've had before is a misrepresentation of the facts.
15 weeks is rather short. Additionally, it's not really 15 weeks. The study time scale starts at the 1st vaccine dose (week 1). Then it's 3 weeks until the 2nd dose and 2 more weeks till full protection. So the actual protective coverage span in this study is week 8 to week 15, or 7 weeks.
This study being held up as proof of long lasting immunity doesn't hold water. It is not bad news though. Decent B-cell responses (though tailing off) till 7 weeks after full vaccination is good. But we definitely need to know what happens after the first 2 months too. This exact study should be repeated again in 6 months (24 weeks).
You're right. It's the lower bound, based on the duration of the experiment.
There have now been many, many studies all pointing in the same direction. A small selection:
https://www.thelancet.com/journals/lancet/article/PIIS0140-6...
Natural infection protects against Covid (incl. Alpha variant). Adjusted incidence rate ratio for covid infection - 0.159 (84% protection) and symptomatic covid - 0.074 - (93% protection) - 7 month follow up
https://jamanetwork.com/journals/jamainternalmedicine/fullar...
Patients who had 1 PCR positive tests had Hazard ratio 0.06 of further positive PCR - 94% protection - 12 month follow up.
https://academic.oup.com/cid/advance-article/doi/10.1093/cid...
After 1 positive PCR, Protection against any COVID - 81.8%, symptomatic COVID - 84.5% - 6 month follow up - protection increased over time.
https://academic.oup.com/cid/advance-article/doi/10.1093/cid...
seropositive patients had 94% reduction in hazard of testing positive - 8 month follow up
https://www.nejm.org/doi/full/10.1056/NEJMoa2034545
Adjusted risk ratio of covid infection for antibody positive healthcare workers was 0.11 (89% less likely) - 7 month follow up period. All reinfections were asymptomatic.
At this point, claiming that immunity to Covid (even against "the variants") is less than a year is an extraordinary claim. There is no reason, prima facie to presume that the results will be different for vaccines.
I'm not sure I agree with just assuming protection will last that long as a default. This study does not establish it but it is a good stepping stone to proving that theory.
re: your edits, the tangential bit from this paper about sars-cov-2 positive cases wasn't the main thrust and from the graphs it looks like their neutralizing antibody levels actually are multiple logs below mRNA vaccinated people at the same 15 week point. I'm not sure what all these citations about naturally infected people add to the topic being debated.
Who is this? Why do we care what he says? Can you provide a source for the quote?
The Cleveland clinic disagrees with your “authoritative” quote (see comments above)
I’d also like to add, I don’t think many ppl are thinking they’d rather get the disease vs the vaccine, rather, if they already got the disease, is there a real benefit vs the risks of the vaccine (eg the heart stuff we’re seeing now). Personally I was careful and never got sick, so I got the vaxx ASAP, but I do think it’s a fair and legitimate concern.
Some people just aren't motivated by fear or shame, and so for a universal campaign to succeed, we need to appeal to those peoples' sense of reason.
Children aren't currently eligible for any vaccine, and some immunocompromised people can't get the vaccine.
I disagree reason is somehow going to overpower the conspiracy machine. Rules and consequences speak directly to those too greedy to vaccinate or are petrified by fear of some conspiracy theorized takeover.
I'm saying it does not justify a relationship where people show vaccine passport ID everywhere they go. Greed is a pretty coarse rationale, I'd suggest it's on the critic to be more persuasive. Conflating the arguments against passports with arguments against vaccination is too disingenuous to accuse someone of, but if someone did't see the difference, it sort of ceases to be an intellectual discussion at that point. So what is the effect?
No, as other commenters pointed out coronaviruses are different from the flu viruses in that they cannot mutate as easily as flu does. Hence it is possible that booster shots will not be required.
If you read any of the articles I've cited one of them has the CEO of Pfizer stating that we will likely need a yearly booster shot.
Nope, and for the same reason COVID deniers who claimed "it's just like the flu" in the beginning were wrong.
I admit I'm not medically trained, but the graph [1] seems pretty clear to me, and the authors said:
> In contrast, participants with SARS-CoV-2 antibodies at baseline before the first vaccine injection rapidly developed uniform, high antibody titers within days after vaccination (median AUC before vaccination, 90 [43 participants];
>at 0 to 4 days, 133 [7 participants];
>at 5 to 8 days, 14,208 [15 participants];
>at 9 to 12 days, 20,783 [8 participants];
>at 13 to 16 days, 25,927 [20 participants];
>at 17 to 20 days, 11,755 [4 participants];
>at 21 to 27 days, 19,534 [14 participants]; and
>after the second dose, 22,509 [19 participants])
[1] https://www.nejm.org/na101/home/literatum/publisher/mms/jour...
Most notably, even those previously infected people with ~0 titers at baseline rapidly developed high levels of antibodies at 5-8 days after vaccination. It's a small group, but the rapid nature of the response is telling.
This data is clear that the infected people had a rapid, robust immune response to vaccination. It cannot tell you what you're trying to infer -- that the vaccination itself increased the immune response. To determine that, you'd need to do some other experiment.
I don't know of any study of the Delta variant (or other recent variants) comparing immunity acquired from infection versus immunity conferred by vaccination -- AFAIK, it's still unknown how these compare and whether a vaccination might provide additional immunity against variants. IIRC, the mRNA vaccines were developed to target key parts of the virus that are thought to be unlikely to mutate without decreasing virus viability.
On the contrary, from all that we know today, wouldn't we expect people with high IgA titres to even develop neutralizing immunity, at least in the weeks after titres peak?
These are all real-world studies of actual duration of immunity. They trump any theoretical concerns based on lab measurements of neutralizing antibody levels.
Observing that the vaccines induce responses lasting as long as 15 weeks is completely unsurprising, based on what we already know from real-world observation of natural infection. Ignoring contextual evidence and concluding that this specific paper didn't provide reasonable evidence is losing the forest for the trees.
Could it be possible that the vaccines don't confer immunity lasting as long as what we're observing from natural infection? Sure, I guess.
Is it likely? No.
We need to compare "1 dose, x days after first dose" and "two doses, x days after first dose" to compare the same thing
Also, to get a better sense of the timeline for vaccination effectiveness, take a look at a chart like this one: https://www.technologyreview.com/2020/12/10/1013914/pfizer-b...
We need something like, 21 days after the first dose, and split the result between people who got one dose and those who got two. We also need to make sure that the repartition of ` age since first dose` is the same for the two doses group and the single dose group.
The park might be full of needles but that's no justification for further litter.
Why do we need yet another database? People have enough problems with the no fly list and that's a short list. A DB that has 1/3 of the country flagged would cause mayhem from false positives and inconsistent data.
I do believe there are others already doing so too, but none of them are open and acknowledged by the public.
The No Fly List and felony registration for gun ownership being 2 examples.
edit: before the downvotes start, agreement with those lists does not negate that they are restricting freedoms based on activities that added or removed someone from a list
You got me there.
I believe the No Fly list is a tragedy of Kafkaesque bureaucracy that I wish didn't exist. People have found themselves on it with little recourse.
I haven't researched the felony registration list enough to speak to it intelligently.
Source CNBC.
[1] https://www.reuters.com/business/healthcare-pharmaceuticals/...
https://www.businessinsider.com/vaccinated-among-delta-death...
I would see two main reasons for this:
- vaccinations are far from "94% effective" in the age groups who need it the most (elderly with weakened immune systems)
- deaths are over-counted (death from any cause within 28 days is counted as COVID death)
Or even the bold points at the beginning?
No fully vaccinated people under 50 died, and the overall death rate was 0.13%.
One hundred and seventeen deaths from 92,029 cases is a death rate of about 0.13%.
Sure, but at least driver's licenses are about public spaces. I can drive on private property all I want without a license.
As for the other systems, I personally don't much believe those are okay either, but that's a much deeper argument than this.
We've been losing our rights since the income tax and probably prior. I just want us to stop losing them at a minimum, but asking for that is viewed as some kind of major indiscretion.
I'm vaccinated and would encourage others to get vaccinated but I am very much against forcing it on anyone.
Antibody titres aren't constant. They increase when your immune system sees an antigen, and decline gradually afterward. In individuals with previous exposure to the antigen, they increase more quickly due to immune memory. This is true for any virus. Decline in circulating antibodies does not mean that your immunity has gone away.
Vaccination is, to a first approximation, injecting a large amount of antigen into someone to induce an immune response. Therefore, data that shows that previously exposed people have faster and stronger immune responses to vaccination are simply confirming what we already know about immunity. It does not mean that the vaccination made the response in exposed people stronger than it would have been otherwise.
Maybe it did, but you can't conclude it from this kind of data.
We agree on this.
> I don't know of any study of the Delta variant (or other recent variants) comparing immunity acquired from infection versus immunity conferred by vaccination -- AFAIK, it's still unknown how these compare and whether a vaccination might provide additional immunity against variants.
I'm not aware of any study of this, either. So far, everyone is focusing on the vaccines.
If half the cases are in vaccinated individuals and only half the people are vaccinated, how can the vaccine be 80%-90% effective? That's a mathematical impossibility.
In the case of the deaths, it might be possible because the vaccinated are far older on average and likely over-counted.
for me, the question is: how can we prevent the virus from mutating enough to escape vaccine- and covid-based immunity with another variant? the answer is to stop the virus from infecting a host in which it can mutate freely and from which it can escape. we don't know these people, so we should aim to vaccinate as many as possible before it finds another person who walks around with the virus for multiple months with no symptoms, accelerating natural selection thousandfold.
Maybe you're in the wrong thread, then?
> for me, the question is: how can we prevent the virus from mutating enough to escape vaccine
Probably not with a vaccine that is not quite strong enough to prevent spread, but simultaneously strong enough to put selection pressure on the virus.
> the answer is to stop the virus from infecting a host in which it can mutate freely and from which it can escape. we don't know these people, so we should aim to vaccinate as many as possible before it finds another person who walks around with the virus for multiple months with no symptoms, accelerating natural selection thousandfold.
The scenario you are describing is the immunocompromised person whose body can't quite kill the virus, but also puts selection pressure on it. Such cases have been described, but whatever mutation would come out of that is not necessarily going to be much more effective at overcoming the defenses of a normal immune system.
The Sars-CoV2 virus will almost certainly stick around and it will keep mutating, even with the best of vaccination efforts. Nature finds a way. We'll have to get used to it.
I have seen no evidence for either of these claims, other than assertions. If you have some, please provide citations.
1. https://ourworldindata.org/explorers/coronavirus-data-explor...
That sounds like hell.
In other words, those who value individual freedom might want to avoid Canada for its over-boarding groupthink and overtly collectivist mentality.
There are many many people who have confirmed positive COVID tests. At least excuse those.
>I think it's a little irresponsible to society to give anyone an out on getting vaccinated.
I think it's irresponsible to require people who most science points to having better protection naturally, to also have to get a vaccine. From this point of view, 2 dose vaccine still have less protection than natural antibodies. Maybe we should require the vaccinated to keep getting more vaccine shots until science shows they're at par with natural antibodies, lowest hanging fruit and all...
The virus is a moving target and what was true of the alpha variant may not be true of delta or downstream. I guess it depends on what you mean by excuse. If you mean allow people to say go on a cruise with a positive covid test as opposed to a vaccination record that seems tentatively reasonable. If you mean allow workers at an old folks home to opt out based on a prior positive test that is unreasonable. If it makes you even possibly slightly less likely to kill the old folks you should get the jab.
The real problem is the grey area created by such a rule. There are probably multiple times as many people who think they have had covid compared to those that have actually had covid that have never been tested. I know people in the US who had an illness in 2019 who are sure they had covid. If you give them an opening they wont let it go. It will surely get ugly.
> If you mean allow workers at an old folks home to opt out based on a prior positive test that is unreasonable. If it makes you even possibly slightly less likely to kill the old folks you should get the jab.
Where is the line drawn? Maybe it would be more effective for people with 2 doses to get a third? What science is there showing antibodies + 1 shot is more marginal protection than 3 shots?
Why would we do that when the vaccines are safer than the actual disease and effective enough to contain the spread?
The study provides evidence that immunity triggered by SARS-CoV-2 infection will be extraordinarily long-lasting. Adding to the good news, “the implications are that vaccines will have the same durable effect”, says Menno van Zelm, an immunologist at Monash University in Melbourne, Australia.
Yes, but don't just take their word for it. Confirmed clinical test should be the bar. I fear if the "you don't need a vaccine if you've had it" narrative gains traction, even if it is undeniably true, it's going to result in the anti-vaxxers lying about having already had the virus, to manufacture another excuse for themselves. If we've learned anything in the last year, it's that any system that relies on people to pinky-swear they're telling the truth will be exploited by a small but significant minority of people.
We are not a collective. We do not have these types of arbiters who will police and decide what is best for everyone. We are a nation of individuals and if you cannot trust people to "pinky-swear" on this matter then how can you trust them to do anything? Including vote on anything? Or reason? Who will make all the decisions for them?
maybe. or maybe the thread is pointless and i'm just pointing it out.
> The scenario you are describing is the immunocompromised person whose body can't quite kill the virus, but also puts selection pressure on it. Such cases have been described, but whatever mutation would come out of that is not necessarily going to be much more effective at overcoming the defenses of a normal immune system.
i'd wager more than 99% of those mutations won't be more effective. i'm worried about the tail risk in the remaining 1%. i don't know how many mutations are needed for the virus to become sufficiently different for human immune system to stop being recognized and this scenario is the best way to find out.
> The Sars-CoV2 virus will almost certainly stick around and it will keep mutating, even with the best of vaccination efforts. Nature finds a way. We'll have to get used to it.
no disagreement about that. in the long run we're all dead anyway. my issue with just letting it run its course is timing and cost - the argument is that it gets much easier much quicker for all of us with the best vaccination effort compared to alternatives.
I don't believe that it's firmly established that natural immunity is as good as 2 shots or natural immunity + 1 shot.
We bought more than enough doses to vaccinate everyone and downsides are small.
Consider a population of 10 million with natural immunity. Let us suppose that vaccination with Pfizer will kill between 0 and 1.
Suppose that 1% would fall ill and 1% of those die. That is 1000 preventable deaths.
It needn't be very much of a difference just 1/100th of 1% to vastly outweigh the risk of a very safe vaccine.
Florida and other states have not had mandates and they’re doing fine per the data.
It seems like we should be optimizing for vaccinating as much of the (non-antibody) population up to a level where the spread of the virus is contained rather than maximizing resistance in the population with antibodies. There must be a threshold at which the low hanging fruit becomes “people without antibodies” rather than “people with fewer antibodies”. I’m not sure it matters if the antibodies are from the vaccine or infection.
> I’m not sure it matters if the antibodies are from the vaccine or infection.
I'm not entirely sure either. There is some research that since the vaccine is just the spike protein, while natural immune response was to the entire virus, that the natural immune response is more comprehensive.
My Canadian friends seem to think that's what their country has turned into, and on just about every front, not just vaccines.
But, they are still OK, because they know we're never given any challenge to great for our spirits to overcome.
Socialism and socialized healthcare frequently gets painted as being anti-freedom but I think that the lack of socialized healthcare infringes more effectively on individual freedoms than the presence of it. In the case of vaccinations - encouraging widespread vaccination (and there is currently and probably will never be a mandate) allows more of the population to act freely. Canada is only behind on vaccinations (and, in total doses administered we're now actually tied) due to the fact that we don't have domestic production facilities which resulted on our dose orders being delayed until America dealt with their domestic population. I don't think that's unfair and I've been pretty critical of the LPC that failed to build out domestic production facilities early into the pandemic but - eh, we work with what we've got.
I think you are projecting what you view as two options in America - either communism or individual freedoms - onto the rest of the world. That is a myopic approach to take when considering all the cultures and governments in the world.
...while ostracized for defending your self-interest?
I'm not saying one is strictly better than the other. It's a tradeoff. As they say in New York: "If you can make it here, you can make it anywhere". The corollary of that might be: "If you can't make it here, move to Canada".
As a person who lived 20 years in Canada and 14 in the USA, I'll take the USA every day of the week--and for the past year I've paid for my own health insurance directly.
Canada's healthcare system is run by bureaucrats who prioritize many items ahead of citizen health.
Here's one example: A family member is a police officer. While I was visiting home, in Ontario, he was hit with some insane shoulder-related pain. This is one tough guy and he was reduced to tears--some kind of nerve damage or something.
The hospital in Canada told him he needed an MRI. And that it would take between 4 and 6 months til there was an available slot. They gave him a prescription for strong opiates to manage the pain during his wait.
I drove him over the border to Buffalo, shelled out $500, and he had his MRI in less than half an hour. The drive was longer than the wait in the radiology clinic.
There are tradeoffs in every situation. I think Canada's healthcare system is better in one exact way: Nobody's bankrupted of their financial wealth due to healthcare. But many many many Canucks are bankrupted of their actual health, their time, their human wealth, due to healthcare.
What happens if you're poor and don't have anyone to turn to for the $500? Will it take the same time to get a free MRI as it does in Canada? Can you get it fro free at all in the US? (Real question, I don't know how it works and am curious)
We don't actually know this. We know it's less dangerous to them thus far. https://www.bbc.com/news/world-latin-america-56696907 https://www.statesman.com/story/news/politics/politifact/202...
The TL;DR is that you may be able to get it for free, but there's a very large proportion of the population that fails to qualify for medicaid and also won't have the financial stability to float $500 out of pocket and, if they happened to get one, wouldn't be able to afford any follow up treatment.
But I totally agree that the US system is an absolute breeze if you've got money to spare.
We do already have long-term data. You would see side effects for a vaccine within six months, and we have been administering it for much longer than that.
The vaccines are safe.
I used to be a close follower of the pharma industry, and you're making it seem like FDA trials happen on molecules and formulations somewhat related to the proposed formulation and then are, like, transitively approved on that hand-wavey basis. This is totally wrong.
For reasons that should be obvious to any engineer that's worked on any kind of even moderately complex system, the molecule that is tested and trialed is the molecule that goes to production.
You don't test "the technology" and then some unrelated other vaccine and then say, there we go, this one's safe.
You test the actual formulation that will go to production. This can't have happened for this yet. The trials are still underway. Unknown risk.
I dunno if you're misinformed or a troll, but that's dangerous stuff to be putting out there.
Vaccines are amazing life-saving tech, and they're safe because of our cultural technologies (FDA trials for e.g.) that make them safe. You can't take all the safety gear out and still get the same safety rating. Doesn't make sense, lol.
In some areas of medicine we can afford to move slowly and we absolutely should - but when it comes to the flu we don't have that luxury.
But there are many parts of this vaccine that is shared with previous ones and the mechanics have been tested thoroughly. The science is the same. There's just no credible reason for those with normal immune systems to delay.
"This can't have happened for this yet. The trials are still underway. Unknown risk."
That's just simply untrue. The trials completed. Read the link.
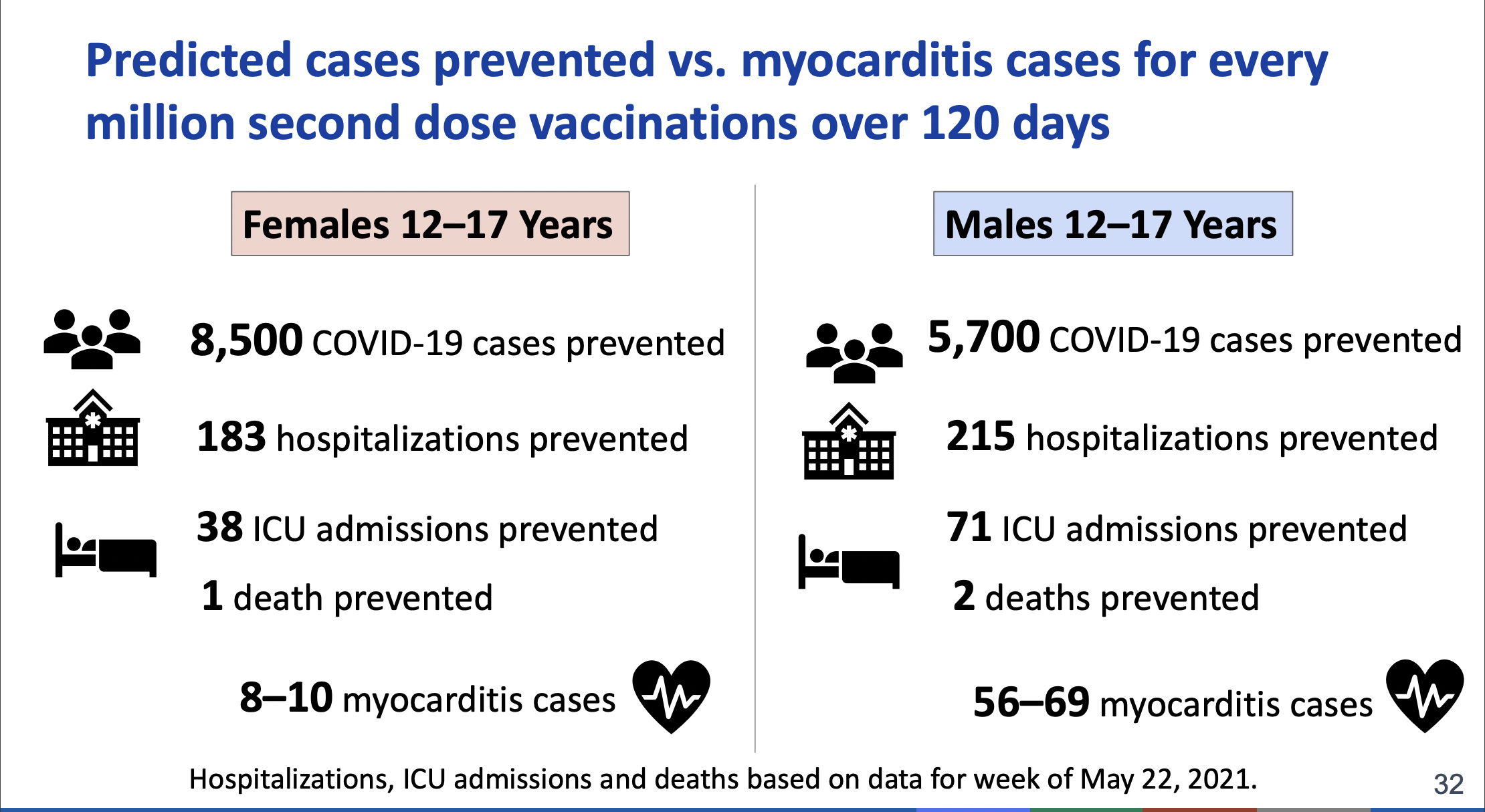
We have now had two separate rare-but-serious side effects of different Covid vaccines: the CVT issue with J&J, and the myocarditis issue with the mRNA vaccines in children. It's disingenuous to suggest that the vaccines are "safe" merely because they've been widely administered; even the question of what "safe" means is a far more nuanced question than you're presenting. For children, in particular, two-dose vaccination with the mRNA vaccines is probably a poor risk/benefit profile. We didn't know that until we started dosing enough kids to see the rare side effects.
The phase 3 trials were not powered to detect rare side effects, which is part of the reason that they're still classified as emergency use, and not fully approved.
I am an advocate for vaccination, but it's not right to ignore these issues.
Safe is always relative. If you don't think the vaccines are safe enough, then please also be consistent and don't engage in equally unsafe activities, e.g. don't drive a car, exercise regularly, eat healthily, don't encourage your girlfriend/wife/daughter/friend to take the contraceptive pill or, even worse, get pregnant, also do not take a large number of other drugs etc.
Again, from what we know today, it is safer to vaccinate your kids then driving them around in a car. Even when the risk/benefit profile is even/negative, absolute risk is super low.
These vaccines are very, very unlikely to give anyone a hard time. Nothing's without risk, but even for the unlucky that doesn't even sound that bad.
As soon as my son is eligible, he's getting it, too.
This is true by medicinal standards, but it's also a sleight-of-hand. The AstraZeneca vaccine had a rare side-effect that was right on track to kill more young women in Europe than the virus itself. That's why it was banned. By that standard, I could argue the viral infection is also safe - for young women at least.
1. https://www.ema.europa.eu/en/news/covid-19-vaccine-astrazene...
The vaccines (being administered now) are safe.
I am extremely healthy, have a great diet, and as a farmer, I get plenty of time soaking up vitamin D, a potent inhibitor of covid. The vaccine doesn't make any sense for me to take.
Normal disclaimer, I am a huge, huge believer in vaccines, and am probably more vaccinated (due to travel and other circumstances) than nearly everyone reading this comment. I believe bar none vaccines are the medical technology that has saved the most lives in our history as a species. Big fan of vaccines.
But, vaccines are made safe via clinical trials and long-term studies. These vaccines are wholly new in type, were rushed to market, have liability waivers for those pushing them, and to make things even worse, the manufacturers aren't collecting followup data about adverse events in any kind of systematic way (as they would during a normal phase4). So it seems to me the playbook that gave us generations of safe vaccines that saved billions of lives has been thrown out the window.
No thanks!
https://www.reuters.com/article/factcheck-covid-vaccines-idU...
They have filed for full authorization for a reason. These vaccines have enough data backing their safety for full approval.
...and if it were choice between vaccinating kids and driving them places, then this example would be relevant.
We don't approve drugs simply because they're less risky for a target population than some other selection of risky things.
> Even when the risk/benefit profile is even/negative, absolute risk is super low.
Yes. So is the benefit.
Yes, if it was a wide-spread problem. The side-effect that killed AstraZeneca wasn't widespread, it was extremely rare, and it was caught because it was such an unlikely combination of symptoms. Yet, this extremely rare side-effect was enough to make the vaccine more dangerous than the virus - to young women at least.
In a year, when all the facts are collected and processed, we'll see how much trouble the Pfizer vaccine really caused in terms of Myocarditis. Then we'll scramble to make up numbers on how many infections must've been prevented by the vaccine to make it all worthwhile.
...like COVID in young people?
It's true that Myocarditis often goes unnoticed and undiagnosed. That's what makes it dangerous. It's a leading cause of cardiac arrest in young people. If you actually do get diagnosed with Myocarditis, it's not necessarily a mild case. That's what makes me suspect the cases being reported now are just the tip of the ice berg.
The chances that a child will experience anything other than extremely minor illness from Covid is also very rare. The current numbers are teetering on the edge of implying that children are at more risk from the vaccine than from the virus.
My definition of the word "safe" includes the rational weighing of risks vs. benefit for a target population. Is it worth it to put kids at risk from myocarditis that exceeds their risk from Covid, just to reduce population-level Covid stats and reduce the marginal risk to the elderly? I don't know, but it's not a question to simply ignore.
Child deaths attributed to vaccines [2]: 0. We can break this down further: 3 deaths from blood clots attributed to adenovirus vector vaccine, none in children. 616 reports of myocarditis[3], 393 confirmed, none fatal.
[1]: https://downloads.aap.org/AAP/PDF/AAP%20and%20CHA%20-%20Chil...
[2]: https://covid-101.org/science/how-many-people-have-died-from...
[3]: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/safety/ad...
Moreover, you're implicitly using a biased selection of data to make this argument. Want more children to die of myocarditis? Keep doing the same thing we're doing now. It will happen. We've been vaccinating kids for a fraction of the time they've been getting Covid.
I will say this for the benefit of others: regarding the CDCs numbers, in particular, they've used the incorrect counter-factual (no doses vs. two doses), and substantially mis-represented the rates of myocarditis in children.
https://medium.com/@wpegden/weighing-myocarditis-cases-acip-...
I've been mortified to see the CDC spreading this kind of mis-calculation so widely. It's simply unconscionable.
It isn't false, though the blanket "it was banned" statement lacks context:
https://en.wikipedia.org/wiki/Oxford%E2%80%93AstraZeneca_COV...
> It is generally advisable to get Moderna/Pfizer if they're available and you're a young woman but the chance of mortal thrombosis is around 5 per one million.
No, the risk for anyone to develop a lethal thrombosis is roughly 5 per million. The chances are much higher for younger women, to the point where it exceeds the risk to die of COVID.
It's not even close, for women age 20-29 the risk of fatal thrombosis is 1:250k, while Covid is somewhere around 1:25k [1]. That's a whole order of magnitude.
The risk/benefit ratio of AZ vaccine is only poor when the risk of exposure is very low [2].
[1] https://www.nature.com/articles/s41586-020-2918-0/figures/2
[2] https://assets.publishing.service.gov.uk/government/uploads/...
I have yet to find a source that gives the risk for that cohort.
> ...while Covid is somewhere around 1:25k
Even if it's an order of magnitude higher, the risk of a actually getting a PCR-confirmed infection is an order of magnitude lower.
Again, Germany: 28 deaths of women in that age group over the course of the pandemic[1], including all potential co-morbidities that may tilt the risk in favor of vaccination.
> The risk/benefit ratio of AZ vaccine is only poor when the risk of exposure is very low.
This is comparing "ICU admissions" against "Serious harms due to the vaccine". Utter nonsense. Why not compare mortality? Probably because it wouldn't look too good...
[1] https://www.statista.com/statistics/1105512/coronavirus-covi...
Please do not spread misinformation, especially misinformation about healthcare during a deadly and dangerous pandemic. Lives are at stake.
Moderna's FDA trial: https://clinicaltrials.gov/ct2/show/NCT04470427 Estimated Study Completion Date: October 27, 2022
Pfizer's FDA trial: https://clinicaltrials.gov/ct2/show/NCT04368728 Estimated Study Completion Date: May 2, 2023
JnJ's FDA trial: https://clinicaltrials.gov/ct2/show/NCT04505722 Estimated Study Completion Date: January 2, 2023
Study completion date does not mean phase 3 trial completion date.
“ However, these dates do not mean clinical trials will continue for this long, and instead reference continued safety monitoring after the vaccine has been approved and rolled out, which is standard practice within the industry”
https://www.pfizer.com/news/press-release/press-release-deta...
Get a clue. Lives are at stake. Vaccination will save them. The majority of people dying now are dying because they made the choice not to get vaccinated.
It is clear that I'm correct. The vaccines are still in phase 3 clinical trials, as reported by clinicaltrials.gov, the source of truth for such questions.
Estimated Study Completion Date literally means the date that the Phase 3 trial study is estimated to be completed, at which point FDA goes through the process of approving or not approving the treatment.
The vaccines have been released due to an EUA (Emergency Use Authorization). I'm guessing you're not aware of this, even though it's clearly elucidated even in your own link.
It seems you think that the actual, you know, "study" part of Phase 3 trials is just some unnecessary bureaucratic technicality thing? As someone well acquainted with the world of pharma, I assure you it is not. It seems you think they just jab the 40k or so participants, watch them a few minutes, and then the Phase 3 trial is completed save for some paperwork. I assure you, that is not the case.
Phase 3 serves a very specific, important purpose: Identifying any long-term safety issues with medical treatments prior to their authorization for widespread adoption in the USA. The reason Phase 3 exists is because it has very often been the case that promising treatments turned out to not be so promising after long-term study.
One of the foundational, bedrock principles of bioethics is "informed consent". That is, the people undergoing medical treatment, especially experimental medical treatment, must have full information about the risks and potential benefits of treatment. You are spreading misinformation which may lead others to misunderstand the current state of the covid vaccines. They are not through phase 3 trials. According to every other situation when treatments not approved through the normal FDA process are administered, they are called "experimental" (e.g., my grandma, prior to her death, was given the option to take drugs that were currently in phase 3 of FDA trials for treating her ailment, and she was told, accurately, that she could elect this experimental drug, which often is authorized for terminal patients--but they are given INFORMED consent--i.e., told they are experimental and the safety risks are not fully understood).
Please, please stop violating bedrock principles of bioethics. These vaccines are still not through phase 3 trials. This is just a plain fact and you shouldn't lie to people to increase their likelihood of taking these vaccines.
The current data we have shows the vaccines are very safe to a high degree of certainty. If you had created a bar beforehand, they’d have met it. But you can always keep moving the goalposts.
All the other vaccines I have been administered had at the minimum a decade of widespread use following their phase 3 trials (and as an aside, their phase 3 trials were much longer studies than these covid vaccines are projected to be).
I've never taken a drug released under EUA.
I investigated every vaccine I took and assessed the risk/benefit ratio and elected to take them. In general, I love vaccines, and I love the medical establishment that gave me the option to elect them! However, the medical establishment seems to have thrown away the playbook on these particular vaccines. The point is, I could examine the risks of those vaccines, and since their administration was not politicized, the data was totally trustworthy. And since most were out of patent, the financial incentive to manipulate data just wasn't there. I could be reasonably informed of the risk. Since these have not completed phase 3 trial, much less have decades of history in widespread use, I have basically no long-term safety data with which to inform my decision. So, precautionary principle tells me: No, thanks!
The risk to benefit ratio is the only thing that matters to me, as I believe it should to others. My likelihood of serious impairment from covid seems very low to me, just like it seems very low to children, for instance. Further, the ratio changes every single day: The more people who get vaccinated, the lower my risk gets, as does the risk for every other unvaccinated person, making the ratio, as more get vaccinated, skew towards not getting the vaccine.
Please stop spreading misinformation during a deadly pandemic.
Moderna's FDA trial: https://clinicaltrials.gov/ct2/show/NCT04470427 Estimated Study Completion Date: October 27, 2022
Pfizer's FDA trial: https://clinicaltrials.gov/ct2/show/NCT04368728 Estimated Study Completion Date: May 2, 2023
JnJ's FDA trial: https://clinicaltrials.gov/ct2/show/NCT04505722 Estimated Study Completion Date: January 2, 2023
You are saying that I am putting people, or society, at risk simply by stating the simple, 100% true fact that these vaccines are not through FDA Phase 3 trials.
The implication of this is you believe it is best if people are NOT given informed consent, that they are kept in the dark, and told lies about the status of these vaccines, because doing so will encourage more people to take them.
I'm sorry, man, but that is just awful, terrible stuff.
Coursera has a course on bioethics, you may want to inform yourself before you engage in discussions about medicine, because you are totally operating in an evil way.
There are lots of things we do see and we should worry about. The problem is that we can't tell right away if it's just noise, if it's a potentially rare side-effect. Then you have the problems like Myocarditis, which are clearly caused by the vaccine, which we hand-wave away with speculative "the benefits still outweigh the risk" scenarios:
https://cdn.arstechnica.net/wp-content/uploads/2021/06/Scree...
this is not handwaving, this is the foundation stone of modern medicine.
Speculative scenarios based on predictive factors that you could just fudge until the result looks "right" to you, those are the essentially quackery.
The data is publicly available for many countries, e.g. here for the UK:
[1] Report on adverse reactions until 16 Jun 2021 https://www.gov.uk/government/publications/coronavirus-covid...
[2] Vaccination statistics https://www.england.nhs.uk/statistics/statistical-work-areas...
Check the table with reports and fatalities by age, and the paragraph interpreting the data. Together with [2] you can calculate the fatality rate for the 20-29 group. In the end you'll end up with a fatality rate for women age 20-19 in the range of 1:150k-300k (quick back of the envelope calculation).
> Even if it's an order of magnitude higher, the risk of a actually getting a PCR-confirmed infection is an order of magnitude lower.
The source I posted is a metastudy, computing IFR based on seroprevalence from many different countries, so PCR tests have nothing to do with it.
I really can't, because there is no information on which age group got which vaccine. The AstraZeneca vaccine has been restricted in the UK for under-30-year-olds as early as April.
Here is a study (Italy) that estimates the risk-reward ratio (fatalities caused vs. prevented) is unfavorable for the entire below-30 age group, including males:
https://www.medrxiv.org/content/10.1101/2021.05.07.21256826v...
> The source I posted is a metastudy, computing IFR based on seroprevalence from many different countries, so PCR tests have nothing to do with it.
This is true, but PCR tests is how we count actual infections and deaths. When calculating the risk of getting infected, IFR alone doesn't help me, I need PCR tests as a metric of how many infections are actually occuring.
Alternatively, I could use seroprevalence: Assuming that seroprevalence is 10% (way higher than in your somewhat outdated source), then over the course of the pandemic, assuming IFR in our cohort is 1:25K, then the absolute risk was 1:250K - roughly on par with the "vaccine fatality" scenario. This is just an example to show that the numbers aren't clearly in favor of the vaccine.
Regardless of whether you think the vaccines are safe, they are quite clearly effective.
Is that what you're implying?
To directly answer your question: I do not think the ethical calculations change one single iota based on any other outside calculation.
You should never misrepresent or elide any relevant information from people when they're about to make a decision about their health (or, hey, ever, in any situation).
It seems you're thinking if we were honest with people about the status of the vaccines, they'd be less likely to take them.
Like, here's the messaging I think is appropriate: Hey, we have some limited safety and efficacy data about these vaccines. The limited, phase 2 information shows that we think they're safe and effective, however, these vaccines have nowhere near the testing and trials that normal vaccines have prior to authorization. As well as lacking phase 3 long-term study, we eliminated animal studies and animal toxicity studies for some inexplicable reasons, so we're flying a bit blind. But we're in the midst of a deadly pandemic. The risk is yours to take.
I think the majority of people would still take the vaccines.
I think you think we should lie to the masses because they're too stupid to handle the truth.
I think that's evil.
The point of principles is to practice them when it's hard, not when it's easy. If you abandon them when it's convenient or during an emergency, you don't really have any principles.
You think you are smarter and more thoughtful about this than the experts who debated it in the open for hours upon hours to decide it was safe and should be available to everybody.
You said earlier you were safe because of your vitamin D levels. The science on the protective nature of vitamin D to COVID is not clear at all. But you claimed it as fact because you want it to be true. You want the vaccines not to be safe so you make up thresholds and then tell us you are being honest by saying the vaccine doesn’t cross them. Why do you trust all the other vaccines the FDA has approved, but not this one that the FDA says is safe and effective. Do you trust them or not? Or do they lie sometimes when you disagree and tell the truth when you agree?
Please stop fear mongering and repeating falsehoods that have been proven time and time again to be incorrect.
https://www.reuters.com/article/uk-factcheck-vaccine-monitor...
https://www.pfizer.com/science/coronavirus/vaccine/about-our...
“ This trial began July 27, 2020, and completed enrollment of 46,331 participants in January 2021. On November 18, Pfizer and BioNTech announced that, after conducting the primary efficacy analysis, their mRNA-based COVID-19 vaccine met all of the study’s primary efficacy endpoints. On December 2, 2020, the Medicines & Healthcare Products Regulatory Agency (MHRA) in the U.K. authorized the Pfizer-BioNTech COVID-19 vaccine for emergency use, marking the first Emergency Use Authorization following a worldwide Phase 3 trial of a vaccine to help fight the pandemic. Shortly after on December 11, 2020, the U.S. Food and Drug Administration (FDA) authorized the Pfizer-BioNTech COVID-19 vaccine for emergency use.”
Key words: met all of the studies efficacy endpoints, (Phase 3 is primarily designed to find EFFICACY), following a worldwide phase 3 trial
EUA does not equal still in Phase 3. Not even remotely correct.
https://www.pfizer.com/news/press-release/press-release-deta...
Key word: CONCLUDES
Your previous comments point to the long development of other vaccines as a mark against COVID-19 vaccines. Surprise surprise, a vaccine developed during a pandemic gets pushed to the front of the line and has full priority, no issues with funding, etc. The speed at which it was passed is not a slight against it, considering it was able to still make it through Phase 1, 2, and 3, and then ultimately gain EUA. Again, not because it was rushed, it still had to go through all other testing other vaccines had, if anything full approval was delayed so they could get 6 months of additional EFFICACY data.
https://www.mercurynews.com/2021/04/29/covid-19-vaccine-myth...
I just think you're taking issue with silly things, overblowing the risks and trying to make other people scared. That's seriously messed up.
Be truthful. You've decided not to take it no matter what. Now you're back-filling reasons not to. If you truly were about your ethics, you'd stop trying to make others afraid because you are.
I have said zero about the safety of the vaccines. I have only stated the unassailable fact that they have not completed phase 3 trials.
How is telling the facts about the status of the vaccines spreading doubt?
I have taken plenty more vaccines than you, I'm sure, I'm not some anti-vaccine nutcase. I love medical technology, I love vaccines. I also love bioethics. I wish more people, like you, did too.
You say I'm afraid, and you couldn't be further from the truth. I'm more well-informed about covid than most people I interact with on a daily basis, and I live in a state that values individual autonomy, so we've experienced basically zero impact on our daily lives because of covid. Some folks used to wear masks, most folks didn't. Everything remained open, save a brief closure of our bowling alley, now thankfully back open.
I walk around without any fear whatsoever and all my local fellows seem to as well. Nobody talks about covid or really cares much about it all. Very few are vaccinated.
Life is fine.
Others are more scared. Others, like you, are trying to hide information about the vaccines. That sucks.
I hope your life improves, friend!
You know nothing about me.
Strange you think we should all be as subservient as you were when you were a Marine. I mean, I get it, I want our armed forces to have a solid CoC that can be relied upon, but pushing it to the point where you have to obey orders to take random needles without any informed consent seems a bridge too far for me. Stranger still is you seem to think this is how we should operate in the civilian world.
The vaccines are safe.
It seems like you're claiming anything that gets an EUA, regardless of FDA trial status or outcome, is "safe".
That would imply you believe FDA Phase 3 trials are irrelevant, and that safety, particularly long-term safety, is easy to assess without doing any long-term safety studies.
That's quite a strange position to take, but OK, you can take it.
I trust the FDA, however. It's strange to be arguing with somebody who doesn't trust the FDA, but here we are. I trust them, and they think long-term safety trials for pharmaceuticals are really important. You seem to disagree. That's fine.
I agree that the vaccines show good safety profiles for older patients in the short term. The younger the cohort it's administered to, the greater the number of adverse events occur, however, which is worrying, because it's the opposite for covid. But still, they look reasonably safe for the 18+ crowd, in the short term.
You seem to think they're perfectly safe in the long-term based on no studies. That's a cool, if strange, way of magical thinking. I think differently, and I seek data and trustworthy sources for my medical information.
For what it's worth my doctor also recommended I don't get the vaccine, for the same reasons I've laid out here.
The OP is throwing around giant misleading statements like "potent inhibitor", while chiding others for incorrectly stating tiny details.
The vaccine is a "potent inhibitor" of COVID, and we all have the data to prove it. There is no other substance, other than monoclonals, which would meet that standard.
The latest meta analysis indicates that ivermectin is also a fairly potent inhibitor, although the evidence is weaker.
There is one medium sized almost randomized trial that shows a strong result. I'm not interested in small retrospective studies. There are 50 retrospective studies that show HCQ is an amazing drug against covid.
Clearly since there is little downside to given vitamin D to people who have low levels, it can and probably should be done, but that is very far from proving that it is a "potent inhibitor" of covid. There also is a clear bias for the person who makes that site since they also want it to be true. Maybe they don't look as hard for studies which disprove what they want. It isn't an overwhelming case.
There is more than enough evidence for a big RCT to actually confirm, but given the safety considerations and low expense it probably makes more sense to just dose everybody and hope it works. But I don't see how you could make grand claims with this evidence.
Super, super strange that we'd take less-than-typical studies of novel vaccines, and then quibble the evidence on something created by nature that we know is easy to get, easy to dose, very safe, etc.
It's like someone wants to make some profit or something.
Do you believe the evidence for their effectiveness is equal?
The evidence about coronavirus is quite, quite clear. There may be long-term severe effects of covid, just like there may be severe deleterious long-term consequences of the vaccines. So you must calculate your risk-benefit ratio and use that to elect whether to take the vaccines or not. For those that are worried about experimental vaccines, I absolutely encourage them to get more fresh air and sunlight--in fact, almost everyone would benefit in many ways from getting outside in the sun, getting fitter, and avoiding prolonged "lock downs" in their houses. (To boot, covid has never been observed in the scientific literature to be transmissible outdoors.)
Here's a peer-reviewed study from the Lancet from this month that shows just how short-term irrelevant covid is to those under age 40 who are reasonably healthy: https://www.thelancet.com/journals/landia/article/PIIS2213-8...
For those under the age of 60, obesity is far and away the thing that makes covid dangerous, and if you're under age 40 and are not obese, the death rate is too low to be measured.
So from that, it seems clear to me: If you're under age 60, get fit (I already am, and getting fitter and fitter every day, which is oddly something never mentioned by the higher-ups at CDC or Pfizer or wherever, which is curious, wouldn't you say?). Get outside.
Effectiveness of the vaccine is irrelevant to me personally because for all people like me covid has thus far posed a risk profile similar to that of driving. Novel vaccine technology presents a totally unknown level of risk, and we've already observed plenty of healthy, young people get all sorts of negative outcomes from it. Plus, again, totally unknown long-term safety profile.
I'm curious why you're so against any kind of solution for covid that doesn't involve novel vaccines.
https://www.narcolepsy.org.uk/resources/pandemrix-narcolepsy
In fact, there are many, many vaccine-related long-term injuries that are well-studied and were totally not detected until well after the fact.
In fact, there's an entire medical school textbook about it, if you want to really know, published by Wiley, called Vacines and Autommunity: https://www.amazon.com/Vaccines-Autoimmunity-Yehuda-Shoenfel...
The corporate press does everything possible to make it seem to the common person that vaccines are the very single medical technology that has zero side-effects and zero long-term safety issues, but that couldn't be further from the truth.
(Wiley is not some crazy conspiracy theory crap, they make legitimate textbooks for colleges everywhere.)
Not to mention, the question itself is biased. You should really ask, Is there any example of an entirely new medical technology (really, three, if you consider the LNP) which post-deployment caused long-term safety issues?
And that would be a resounding yes.
And, please again note, even knowing all I do about all those things and the dangers of vaccines, I still am more vaccinated than you, having taken, e.g., rabies vaccine, even knowing the not-insignificant risks involved.
However, there was a risk I'd catch and be injured by rabies.
There's almost zero risk I'll be injured by covid, lol.
I mean, as well, look at the injuries being caused by the vaccines: They happen to people like me, young and healthy. Covid only hurts the fat people my age. Why would I take the side of the risk that hurts people like me?
I said show me one where the onset is hidden until after 6 months. The narcolepsy link above was concentrated in the first 6 months after the shot. At least try me with the dengue vaccine and ADE so I could explain why that is different.
Hundreds of millions of people have taken the vaccines and we know with huge amounts of power the side effects and their (incredibly tiny) probabilities. It is beyond uncommon for a hidden side effect to only appear later, especially with something like a vaccine. It produces an antibody response and goes away. If that antibody response is going to cause problems it generally happens sooner than later when there are the most antibodies.
I, like you, didn’t want to be the first person to take the vaccine. But at this point the safety record shows it is one of the safest, if not the safest, vaccine ever produced. Hopefully you don’t get COVID in the meantime of this point becoming clear to you.
{kind=link}
{kind=link}