https://news.ycombinator.com/item?id=37057135
(50 points/3 days ago/51 comments)
Edit: It also ought to be noted that the study was on mice that had been given amphetamines to mimic psychosis. Which is interesting and good science, but seems far from enough evidence for the press to write stories with headlines like "Everyone Was Wrong About Antipsychotics" or "Schizophrenia Drugs May Have Been Off Target For Decades, Study Finds."
This sort of internet story bothers me because I've spent time around schizophrenics who are recovering from a psychotic episode. Schizophrenia can get really, really bad, in a way that I don't think most people who haven't had contact with the psychiatric medical system understand. Antipsychotics have awful side effects, but for many people the alternative is uncontrolled psychosis, which can be vastly worse.
There's a decent chunk of people who inherently and vocally dislike psychiatric medication, and these media stories are in that tradition. But the only people who ought to be involved in the decision about using antipsychotics are the patient, their family, and their medical providers. Writing headlines that are too broad for the evidence that supports them does not help improve the lives of people with schizophrenia.
It's perfectly normal to wonder how can one administrate something when one doesn't understand it. Especially when there can be such debilitating effects.
In clinical settings, things are way less clear than you make it seem. All psychosis are not equal and even all diagnostic of a same patient are not equal.
There is a lot more caution that should be advised. Including in the administration protocols instead of handwaving and just claiming that it should be taken life-long (which betrays that it's not a cure).
It does not even make sense in the first place that there is no attempt at finding the base neuro-transmitter levels in and out of psychotic phases for each patient before deciding on the posology of a treatment. Managing plasma concentration in a finer-grained way might avoid some (not all) of the issues with neuroleptics.
Some people even only have a few episodes every few years and are still put on life-long treatment with all the side-effects that can then be seen.
It needs to be way more fine-grained if not restudied.
A theoretical/principled understanding of how a drug works has never been required for useful medicine to happen. For example, we don't know how general anaesthesia works. We don't know why some people have extremely bad reactions to certain anaesthetics (and they do). And yet they are used every day, to enormous net benefit.
> finding the base neuro-transmitter levels in and out of psychotic phases for each patient before deciding on the posology of a treatment
Is it actually possible to measure that, non-invasively?
I think, on the first question, the public conversation about schizophrenia is not ideal for improving outcomes. In particular, people in their 20s who have a first psychotic episode need to be pushed by their friends and family to get medical care immediately. Schizophrenia treated early is associated with much better outcomes later in life, and long periods of untreated psychosis are associated with much worse outcomes. I think that poor quality articles like this one sustain that section of the population who distrust psychiatrists, which leads some schizophrenics to seek treatment too late or not at all.
On the second question, I think that doctors are doing about as well as they can with antipsychotics with the current state of knowledge. Though it sounds like your concern about overprescription is from experience, and my feelings about the right level of long-term antipsychotic use are much weaker than my feelings about the public conversation.
I agree that it would be better for antipsychotics to be better targeted. Measuring individual neurotransmitter levels sounds like a very interesting way to better target treatment, though I don't think it is straightforward to measure neurotransmitters in a living brain.
I agree that many patients are on antipsychotics for longer than is necessary. The challenge is distinguishing between patients who should discontinue antipsychotics and the patients who will immediately relapse into psychosis without meds.
---
Other thoughts:
> It's perfectly normal to wonder how can one administrate something when one doesn't understand it.
This is a mischaracterization of the state of the science. Antipsychotics are well understood, though not fully understood. We at this point have decades of data on the efficacy of antipsychotics, the prevalence and severity of side effects. We know most of the interactions between the drug and the body. What is not well understood is the exact mechanism by which these interactions moderate psychosis.
> there is no attempt at finding the base neuro-transmitter levels in and out of psychotic phases for each patient before deciding on the posology of a treatment
To my non-expert ears this sounds like an interesting approach to make treatment more targeted. I am not aware of a technology that could currently be used to measure neurotransmitters in a living brain, and I worry that measurement would be invasive.
> Some people even only have a few episodes every few years and are still put on life-long treatment with all the side-effects that can then be seen.
And that would be a more accurate understanding of it - and I hope its true. Current antipsychotics are helpful but imperfect.
"The findings also offer a glimmer of hope that researchers can correct course and use these new insights to design much-improved treatments for schizophrenia. Treatments that can't come soon enough."
Close enough, right?
Journalists know how to write headlines that make people read the article, or at least some people. They are little dramas, and if you start by giving the plot away like that, as if you just simplified a scientific paper a bit, your analytics will tell you to look for a different job soon. It is what it is. So no, it couldn't 'just as easily' be this alternative thing if it wants to get attention.
And I don't think this is always a bad thing. It only gets bad if the headline is overly editorializing, clickbait or just plain false. I don't think it is in this case.
If we understood what’s really happening we could target pathways better.
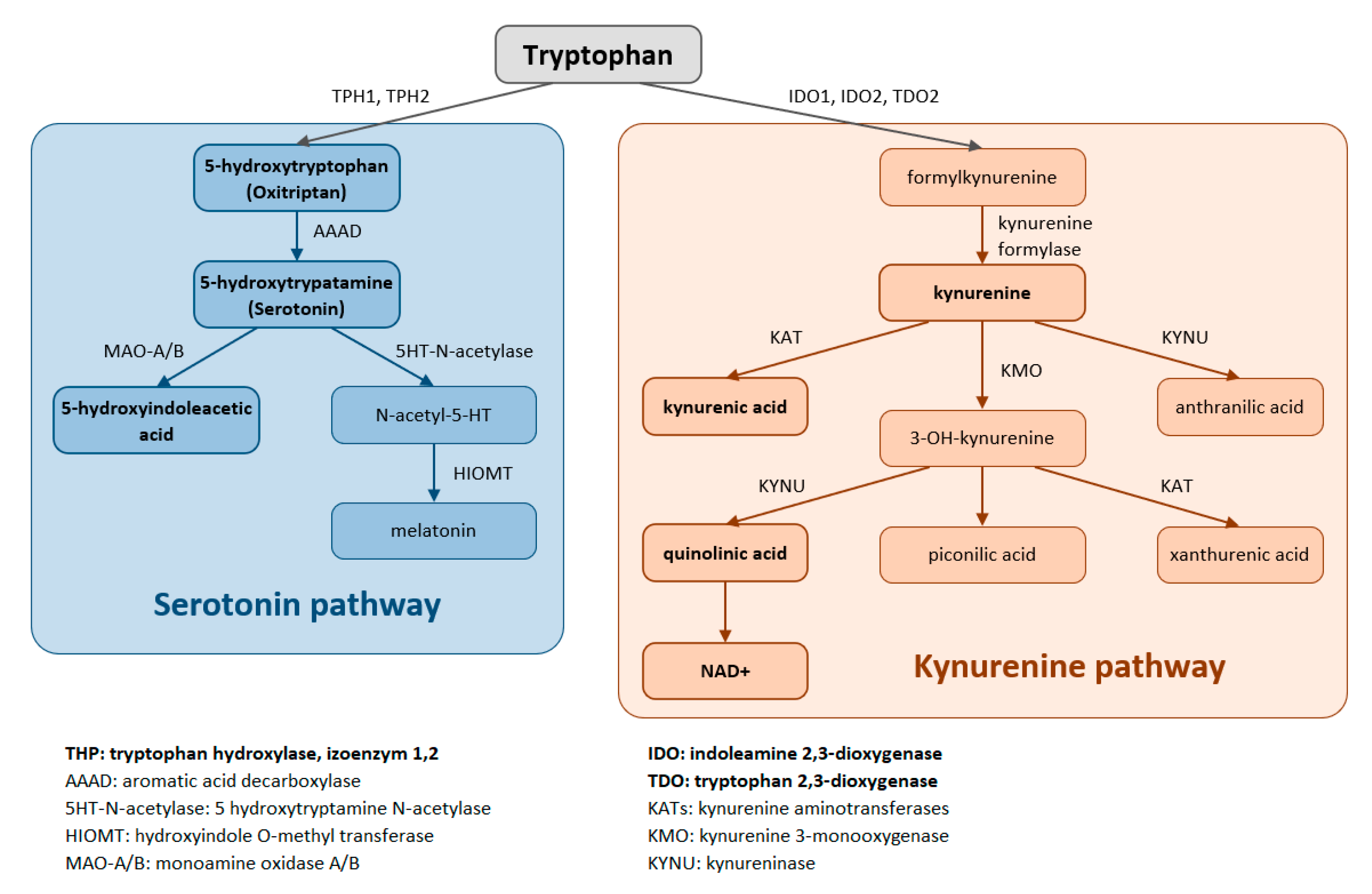
https://www.mdpi.com/ijms/ijms-22-11714/article_deploy/html/...
My mood disorder is caused by an immune disorder. How do I know this? When I take TNF Inhibitors my mood disorder goes away. But it is all over my genetics (PNP, CACNA1C, EARP1, TNPAIP3, SLC18A2, SLC1A2, SLC23A2 are the most relevant) and I have found rescue in high dose zinc and ascorbic acid not only for my mood, but also for my Ankylosing spondylitis.
Note as well that I had my worst paranoid delusional states both time I had COVID.
Here is a tip from a two time suicide survivor; Doctors can only treat the symptoms, and most do its poorly. Use medicine to get stable and stay alive but figure out the rest on your own.
The headline is a bit attention grabby perhaps (and of course, that is what a headline must do), but I wouldn't even call it clickbait. It is even fairly accurate. Yes, they were likely off target with the specific neuroreceptors, no that doesn't mean the medication didn't work and of course, this is a positive development for designing better medication. This is classic storytelling, draw the reader in with some conflict and save the resolution for the end.
We need to be able to discuss negatives and limitations associated with psychiatric medication in an honest and nuanced way. They often don't work well enough, there are costs associated and just giving somebody a pill and be done with it is hopelessly inadequate to the point of negligence.
As someone who did experience uncontrolled psychosis myself, let me tell you the absolute taboo of discussing these matters made me way more uncomfortable than the side effects. Furthermore, psychiatry made me feel like a diseased animal at times, not to be taken very seriously and just put on drugs for life to be on the safe side. In hindsight I do appreciate how difficult that line of work is, doesn't change my experience.
I am not against medication really, actually I think they are a must-have. I just think most anti-medication people are not really rallying against the side effects or at least not initially, but grew opposition out of bad experiences with treatment that focuses only on medication and was just very inadequate. Medication is what represents that. Additionally, medication can come to represent your loss of sanity and with that, you fundamental not-belonging to the group of 'normal people'. Thus the desire to not be on meds 'for life'. Haven't spoken to a single therapist or psychiatrist who made me feel that was a legitimate desire and who understood that. Maybe things have changed, this was a long time ago.
To deal with the resentment against meds, I think it is way more effective to address those concerns directly and without fear, rather than putting down everything that might be interpreted as negative about medication.
Like you say, without experience yourself, you have no idea how bad psychosis can get. It is a really complex thing and you will need much, much more than pills. And not only for the psychotic episodes, because these experiences tear at your identity as a human being. It isn't over when the psychosis is over.
Consider the discovery of valproic acid:
"Valproic acid is a carboxylic acid, a clear liquid at room temperature. For many decades, its only use was in laboratories as a "metabolically inert" solvent for organic compounds. In 1962, the French researcher Pierre Eymard serendipitously discovered the anticonvulsant properties of valproic acid while using it as a vehicle for a number of other compounds that were being screened for antiseizure activity. He found it prevented pentylenetetrazol-induced convulsions in laboratory rats. It was approved as an antiepileptic drug in 1967 in France and has become the most widely prescribed antiepileptic drug worldwide. Valproic acid has also been used for migraine prophylaxis and bipolar disorder."
To this day, nobody knows exactly how it works, apart from the fact that it hits more than a few targets. (And it's a particularly potent inhibitor of the epigenetic modulator histone deacetylase.)
Apart from a subset of very clear-cut cases -- steroid hormones, peptide hormones, and certain aggressive chemotherapeutic drugs -- there's no clear model for most small molecule drugs. Even really mundane ones like metformin and paracetemol are very imperfectly understood.
That doesn't mean it's a useless result, but everyone should remember that research is an accumulation of decades of many little pieces of information. This is another clue, not a "nail in the coffin" of old theories.
The ultimate evaluation of medication is how well it actually performs in studies. If someone can develop a new medication that is more selective for D1 and show that it performs better and/or has fewer side effects then this would be a great result.
However, don't get too excited. The pharmaceutical industry is often 10 steps ahead of public findings like this. A selective D1/D5 antagonist with negligible D2 affinity has already been trialed for schizophrenia without good results: https://en.wikipedia.org/wiki/Ecopipam
Many of the most prescribed schizophrenia medications already have significant D1 affinity, too, so it's not really correct to say that we're "off target"
These findings tend to be very aggravating to computer scientists who are familiar with systems that (mostly) obey clear-cut rules and can examined in extremely fine detail with enough equipment and motivation. Neuroscience is not so simple, but that doesn't mean it's all wrong. Each finding is one more piece of the puzzle.
The only things those drugs did to me were making me comatose, poop my pants, sleepy, dumb and hungry.
You can't be declared psychotic or paranoid, when the only thing you can do is sleep, drool, poop yourself, and make 3 words sentences, so lazy doctors think these drugs work.
But they don't, there was zero change in my beliefs, fears, anxieties, I was the exact same person, only slower, dumber, and sleepier.
And at some point, when you're exhausted from being a zombie, you end just lying to your doc and pretending everything is fine, even when you believe doctors should always know the truth, because it's the only way to stop yourself from staying a brain dead zombie for life and causing irreversible damage.
So I have to lie to doctors to steer them towards the care I really need. I would prefer not to lie. I tried not to lie. But when you tell them you want to quit or go as needed, they gently suggest committing you or lose interest in you. They see you as a toy to experiment on. It's impossible to be treated like an adult. It's infuriating.
I realise a sample size of one anecdotal piece of evidence is hardly scientific, but I’m getting rather tired of the constant mouse model studies, with barely related parameters.
I wish there was a better way to do medical research, in actual human beings. Unfortunately it seems historically that actual human medical research is mired in the suffering of the (generally unwilling) participants.
Serious point, maybe schizophrenic symptoms are cause by a disruption in REM sleep. As in the suffers are experiencing a waking dream. Some time back they did an experiement on students and kept them awake for days-and-nights on end. Eventually they couldn't tell the difference between the dreaming and the real world.
I've experienced severe psychosis. For me, it was a merging of reality and imagination. I always knew what was real, but my brain couldn't filter and ignore the unreal. I would act as if imagination was reality though I knew it wasn't.
Several people I've talked to have said similar things.
I think of dreams as the result of rebooting the brain mid-defrag. It's chaotic in some way. My experiences with psychosis was far too structured and self-consistent to be a dream.
My theory is there is an active component to psychosis that doesn't fit in with REM sleep as a cause.
Kind of like sleep function on laptops. Otherwise, the brain cells would "overheat".
Human sleep would be more aptly related to garbage collection and indexing - neither of which occur when a laptop sleeps. When a computer overheats it throttles performance and sometimes shuts down.
Mental distress/disorder cannot be treated properly because of the strong for-profit motive (unrestricted greed) that these privately-owned (sometimes publicly traded) mental hospitals and pharmaceutical companies have.
Mental hospitals are effectively a prison. Locked doors, removal of rights once committed, coercive and sometimes forced treatment and restraints, being told that you have a lifelong disease (with no measurable physical damage -- fMRI scans are not indicative of damage) that needs drugs for the rest of your life, and getting billed an exorbitant amount - to name a few things that are wrong.
If your rights are violated and you are declared incompetent (which is pretty common if you are unstable or in crisis), it's an uphill battle in special courts called Mental Health Courts. It's difficult to get a second opinion from a third-party psychiatrist, or to contest treatment orders (such as mandatory intramuscular antipsychotic injections or ECT which respectively have a very potent and long-term effects).
The conversation needs to be shifted towards the Soteria House paradigm.
This article sums this model of care pretty well: https://www.madinamerica.com/2019/09/soteria-house-heal/
They have very impressive results, particularly in regards to schizophrenic and psychotic patients, and do not use life-long tranquilizer prescriptions to achieve their results. It needs more study, it needs more implementation, but the core of the model is that it builds a supportive community around vulnerable people -- instead of caging and viciously profiting off of these people.
I spoke on this matter in the past, and you can read my thoughts here: https://news.ycombinator.com/item?id=34029719
Not to mention, weight gain leading to type two diabetes, thyroid problems leading to fluid retention in the legs and memory loss. Not much of a cure :(
Most organs are composed of one or only a few types of cells and their particular arrangement doesn't matter that much. For example swapping kidneys between people doesn't change who they are (mostly, smaller edge conditions apply here). But we can't swap brains because the brain encodes your 'youness'.
Mechanical damage to parts of the brain can cause personality changes. Multiple neurological syndromes are directly linked to macroscopic brain changes. This includes schizophrenia, traumatic brain injuries dramatically increase its risk.
We also know that schizophrenia almost never happens along with epilepsy. They are almost mutually exclusive.
It's fair to say there is no single macroscopic trigger for schizophrenia, but that's it.
Schizophrenia is directly linked to dopamine. So is ADHD, but in the opposite way (not enough dopamine). Both were demonstrated on fMRI.
Psychosis is a physical issue in the brain (too much dopamine making the brain fire when it shouldn't) that's solved by administering dopamine antagonists (= antipsychotics).
My dad developed severe mental illness later in life, destroyed his life, and never found a regiment that worked for him before his death (undiagnosed congenital heart condition is what ended up getting him).
I think anyone who has schizophrenia or bipolar (and their loved ones), would happily take medically "managed" psychosis over the hell of unmanaged psychosis
There's drugs that reduce or eliminate hallucinations for many schizophrenics, so it's something you can treat (except in unfortunate situations like your dad or my uncle). There's a big difference between a medication that actually removes the symptoms over one that sedates a person, they're not the same and one is obviously preferable.
There hasn't been enough concern about how the drugs work, or why they often cause serious side-effects like tardive dyskinesia. It's simply enough that the person becomes manageable for others.
These drugs have been around for a long time and only now is someone investigating deeply into how they actually work.
but also, if you've had a conversation with someone in active psychosis, vs. on the right dose of medication, there is a really incredible distinction in the clarity of their thinking and speaking -- night and day sometimes. so the drugs do work at genuinely treating some of the problems. and good psychiatrists do look carefully for this kind of improvement.
Surprised no mention of pimavanserin (which doesn't act on dopamine useful in those with Parkinson's and psychosis) and that L-dopa can reliably induce psychosis (used on Parkinson's).
https://www.mayoclinic.org/diseases-conditions/serotonin-syn...
All the effective anti-psychotics seem to have anti-serotonin properties, in addition to their anti-dopamine effects. For example: "there are also recent studies that 'stumbled upon' the 'shocking' evidence that anti-dopamine drugs commonly used for treating schizophrenia such as haloperidol are actually potent serotonin antagonists as well." - http://haidut.me/?p=1297
One of you quoted my essay Cargo Cult Psychiatry in a comment on Sunday, on a submission of Feynman's Cargo Cult Science. I responded, then thought to submit my link to the original at Mad In America again: https://news.ycombinator.com/item?id=37110874
This paragraph from that comment is essential for helping anyone diagnosed with the label of "schizophrenia":
"The good news from the mental health world is that Chris Palmer, M.D. published Brain Energy [0] last year. I haven't read more than excerpts from google books [1]. My understanding is Dr. Palmer was a conventional palliative psychiatrist, then he had a patient whose schizophrenia improved on a ketogenic diet. The patient was able to discontinue antipsychotics: Dr. Palmer's mind was blown. Then he discovered the 70+ years of research establishing that mental health conditions are metabolic problems that can be successfully treated with pro-metabolic therapies.
Perhaps the most bold and disruptive
aspect of Brain Energy is understanding
precisely how and why medications that
harm metabolism might reduce mental
health symptoms.
The long-term consequences are of great
concern and require the urgent attention
of the psychiatric community.
[0] https://brainenergy.com/ / [1] https://books.google.com/books?id=FoxlEAAAQBAJ&pg=PT233&dq=B "
> Consider valproic acid: For many decades, its only use was in laboratories as a "metabolically inert" solvent for organic compounds
> Dimethyl sulfoxide (DMSO) is the most common organic solvent used in biochemical and cellular assays during drug discovery programs.
> Despite its wide use, the effect of DMSO on several enzyme classes, which are crucial targets of the new therapeutic agents, are still unexplored.
> 1-4% (v/v) DMSO, the commonly used experimental concentrations, showed ∼37-80% inhibition of human acetylcholine-degrading enzyme, acetylcholinesterase (AChE)
Oops! How many investigations on specific drugs were in fact showing mostly the results of what happens when interfering with one of the most ubiquitous-yet-underappreciated signalling systems, the cholinergic system?
I’m hoping widespread & systematic application of modern methods like in-silico molecular docking studies will lead to much fewer such oversights.
Goes to show a lot of clinical medecine is about short-term relief and not necessarily about real health.
If you really look at it with unbiased eyes, between elective surgeries and what not, it's not really about curing any true dysfunction sometimes. Perhaps too many times.
We just go with the flow but, heck, MDs are not even necessarily healthier than you, some even smoke to this day!
Go figure...
Also there's a huge chasm between lab grade amphetamine and street meth.
Over-medication is a big problem, but you have to recognize that you are extremely lucky to be able to function without it. Not everybody can. I couldn't.
I share your experience regarding side effects, it would likely kill my career. Thankfully anti-psychotics work quickly, unlike antidepressants. As long as I have the discipline to recognize the signs, I can medicate mostly as needed. But this, again, is a privileged situation. More severe cases can't risk that "as needed" treatment.
Or is schizophrenia a spectrum very much alike as autism?
Consider: you can hear voices and choose not to respond to them. You can have delusional beliefs and not act on them. There's no functional difference between talking with your mom on the phone and talking with an alien that has replaced your mom on the phone if you're willing to play along or simply acknowledge "hi schizophrenia, funny idea, that".
It is exactly that. There are a lot of people with pcychosis-related symptoms who go about their lives without treatment.
They experience attacks once in a blue moon, but that is just about it. A few calming words or moments alone help.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6852683/
"Patients with schizophrenia without comorbid substance abuse have only a slight increased risk of violent crime compared with the general population, suggesting that substance abuse plays a mediating role."
And yes, washing hands is common practice now.
Pimavanserin has a unique mechanism
of action relative to other
antipsychotics, behaving as a
selective inverse agonist of the
serotonin 5-HT2A receptor, with
40-fold selectivity for this site
over the 5-HT2C receptor and no
significant affinity or activity
at the 5-HT2B receptor or dopamine
receptors.[2]
That's a very important distinction in the latter part. They are somewhat understood in their action mechanisms, whether VMAT1, VMAT2, D1, D2 receptors etc. But not really in their effectiveness (which is slightly more important, especially to determine administration protocols).
Which is also the point of the article.
So, not that wrong as you might think.
Note that "attributable" doesn't mean causation, but in reality it usually indicates it to some degree.
What I said is still exactly on point.
It's also treated with the utmost care and in most interventions, if there is a choice to do without, the patient is offered the choice. There is a lot more consent involved.
So it's not the same thing.
To answer your other question, yes, neurotransmitter levels can be measured in the blood or urine.
For someone under-treatment, it would only make sense to. Wait 4 or 5 times the half-life of the molecule. (that's the difficulty since once started, they are not even supposed to stop).
This is notably untrue. General anaesthesia is associated with higher risks of dementia. Especially the older the person being treated.
While there's some disagreement here - short term cognitive decline is inarguable as a side-effect (called post-operative cognitive decline), and many suspect it's related to long term cognitive issues:
---
From: https://www.alzheimers.org.uk/about-dementia/risk-factors-an...
> There is a link between surgery and short-term changes in thinking and memory, called post-operative delirium or post-operative cognitive decline. This condition particularly seems to affect older people. Some studies have also found that these short term changes may be associated with higher risk of dementia later in life but other studies have found no association.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6852683/
That isn't to say that schizophrenia necessarily causes the violent behavior: the two variables might not have any causal relationship at all. But the correlation is there.
Even during my first episode, which was by far my worst while having the least experience, I was aware that what I was experiencing (hearing voices/feeling watched) was likely me experiencing psychosis. While I still 'went along' with the episode, I was doing everything in a way that minimised harm to myself and others. I eventually called an ambulance, thinking that either I'm going through psychosis (and need an ambulance), or what I was hearing was real (and having ambulance/police on scene would help).
Once the ambulance arrived I had 'confirmation' that I was going through psychosis, and could then 'ignore' the voices to the point that I wouldn't act on whatever I was hearing. My symptoms continued for a couple weeks, but at no point did I even consider these to be real (despite them feeling very, very real).
Going forward, I've had a couple other episodes, all of which I've noticed early on and been able to act accordingly (reaching out to friends or professionals). While some of these episodes were equivalent in intensity to my first episode, none of them had me acting on the symptoms (beyond calling my psych and saying I'm having an episode).
I was briefly on anti-psychotics, but as I'm yet undiagnosed, my psych wasn't comfortable with me being on them long term. Instead I've been able to manage it through exercise, sleep management, mindfulness, and better management of my anxiety.
That said, I'm only discussing my own experiences with psychosis/potential of having another episode. I'm not medicated but don't worry about it (potential harm to myself or others) in my day to day, though I make sure to mention it to those that could be affected (flatmates or friends/family).
I remmember hearing voices a few times, but they would not last more than a day.
They were telling me to reach out to one person (that would be awkward at the time) or to harm someone close. I've felt fear but knew those voices weren't real.
The voice sounded like me talking to myself.
The other form of voices I get, which are much more frequent + longer lasting, sound like my internal monologue. They can be different voices, but always sound like I'm 'thinking' them (rather than overhearing). These tend to last 2~ weeks after an episode, and come back when my anxiety or insomnia gets worse. Luckily these are pretty ignorable, if not a helpful sign that I'm nearing an episode. I'd compare them to anxious/intrusive thoughts (though a bit more intense).
I haven't had an episode in almost a year and have learnt to easily manage the intrusive thoughts (/possible start of an episode). This hasn't even impacted my lifestyle all that much, if anything it's taught me to manage my work/life balance.
It's like trying to diagnose and treat a political crisis by observing telephone connections. We see stark changes in telephone use in a crisis. If we meddle with the telephone exchanges we might improve or harm various types of event. It's not really about the telephone calls though, we are just hacking at the messaging of an external event we are ignorant of.
A conspiracy theory induced panic might be superficially "solved" but cutting all the the phone lines. We have not identified or solved the cause though and people don't find life without telephones (dopamine) worth living so they plug them back in (quit their anti-psychotics).
But currently we're unable to image live people at that resolution, not even dead people yet.
https://sci-hub.ru/10.1001/jamapsychiatry.2020.1941
The citation is:
Weinberger, D. R., & Radulescu, E. (2020). Structural Magnetic Resonance Imaging All Over Again. JAMA Psychiatry. DOI:10.1001/jamapsychiatry.2020.1941
The article is a follow-up editorial on an older (2016), more substantive critique of MRI methods in psychiatry, which is also worth digesting slowly:
https://ajp.psychiatryonline.org/doi/10.1176/appi.ajp.2015.1...
The citation is:
Weinberger DR, Radulescu E. Finding the elusive psychiatric “lesion” with 21st-century neuroanatomy: a note of caution. Am J Psychiatry. 2016;173(1):27-33.
The situation is about as bad as it can be: there are so many potential sources of confounding in MRI studies that they simply cannot be trusted to say anything about the basic cellular elements of brain tissue in either healthy or diseased patients. All they can validly talk about is themselves; in other words "rather than referring to differences as evidence of brain structural abnormalities, they should be called differences on MRI measurements."
This is without getting into other hugely problematic aspects of MRI studies in mental health: tiny samples; failure to replicate; and most interesting to me, the fact that experimental subjects (i.e. the people in the study "with ADHD" or schizophrenia or whatever) are not screened for psychiatric medication use, which, because medications can shrink brain tissue, can make it look like the condition is affecting brain structure when in fact the drug is. (So another source of confounding, then.)
The drugs are literally have serotonin in the name.
I still hear people regularly refer to mental health problems being due to a "Chemical imbalance", often as a way to defend their use of pharmaceuticals and dismiss the efficacy of any other intervention. It's that they see people justify a non-falsifiable in the efficacy of the current course of treatment. It's that it's hard enough to convince people who have been on SSRI's for decades and are doing badly to take a month to ween off them, a month to see how things go, and a month to get back on them. If they believe their brains are fundamentally broken without evidence it's just about impossible.
It's that when a sixth of American women have taken anti-d's in the past month, and the most popular explanation as to why is they have broken brains that need to be treated with medicine, as if their problems must all be due to some genetic issue or whatever, I find it abhorrent.
I don't know, it pisses me off that these drugs are popular largely due to a mythology and how difficult they are to stop more than they're efficacious is all (not that they are not efficacious). It's not that psychiatrists don't know this theory isn't true, I'm well aware the theory has been well known to lack support for a long time in medical circles, it's that they don't effectively inform their patients.
Medicine should stop calling them "SSRIs" if the SSRI part is a tangential side-effect, better educate patients on the fact that medicine doesn't really know why the drugs work, or even if a given patient will respond to them better than placebo. Governments should ban pharmaceutical advertisements because they make people sick and misinformed.
What should SSRIs be called if the SSRI part is how they work indirectly? What would you call them now? And SNRIs? And MAOIs?
…and by basically the entire general public. Big pharma did a great job on the “depression is a just a chemical imbalance…” awareness campaign, but absolutely dropped the ball on the “actually we were wrong about that” campaign, so that’s still what most members of the public tend to believe.
For ADHD, stimulants actually do treat it by fixing "low dopamine"… in specific areas of the brain. But "low dopamine" is also a description of Parkinson's disease.
But SSRIs don't work like stimulants do; they take a lot more than half an hour to take effect. We don't actually know how SSRIs work in the people where they do work.
Sorry, need to be an anecdote for you. Prozac makes me manic in about 5 hours. We know how SSRIs work, the problem is they are treating a symptom not the cause of depression which is immune dysfunction.
If SSRIs did not increase serotonin there would be no risk of them causing serotonin syndrome, and they do.
What you said is: "[anaesthetic agent] has no observed side effects in general" and that's just not true.
As an aside - my grandmother had hip surgery at 86 and was never the same mentally afterwards. She could walk, but she couldn't remember who her family was. It was not particularly unexpected (she had an existing diagnoses of alzheimers) but the change post-surgery was notable enough that the entire family discussed it. It was like she had been slipping a bit, but the surgery threw her off a cliff. The difference between knowing who you are, but discussing the weather every half hour or so, to having no idea who the people around her were.
Personally - I would firmly place anesthetics into a fairly risky category of drug that we have a very poor understanding of. Which is decidedly not where you are placing it.
Yet your comment said "and has no observed side-effects in general."
Maybe it's my fault for not being specific but in context, I was talking about long-term, possibly irreversible complications. While what you point out exists (every psychoactive drug has undesirable side-effects in general, even coffee can be dangerous), it is incomparable to the rate of occurences of side-effects such as tardive dyskinesia for neuroleptics for instance.
That's why I also added "in general" ...
How is significantly increased rate of dementia among the affected population not long-term? It seems irreversible too?
Yeaaaaa that's gonna be a serious "citations (plural and trustworthy) needed" from me there
https://www.nature.com/articles/s41398-023-02445-y
Here are the plurals….
https://scholar.google.com/scholar?as_ylo=2019&q=immune+syst...
If this is your best citation, then I don't know why you expect everyone to know about and be confident in this theory. And that's without even questioning whether bipolar and depression are the same thing.
Your search results are all over the place and don't show anything coherent.
There is no formal causality link here.
Unless you can find other studies. And even then, methodology matters.
There is a realm of difference between that and the type of side-effects that were the subject of the initial conversation, to the point that I'd be tempted to say it is a red-herring.
From a random sample of HN user's comments in the last year in some context or another this is a well established usage in a supermajority of them. So if you must insist on it, you likely will always be outvoted, at least with other HN users.
If it's about statistics and sampling methodology, I am afraid we are veering toward being quite off-topic.
I'll say that my comment was toward paying attention to the different kind of study methodologies, such as metanalysis vs randomized controlled trials and even within the latter, there are differences in qualities depending on how the control group is ensured. As opposed to experimental groups as well.
Then of course sample size.
All that because cross-correlations are possible and correlation is not causation in general.
So yeah, in the end one can ask on hackernews but that will not be statistically relevant. Worse there is the bias that people who have undergone such procedures without issue won't report most likely. So really that's not a way to collect scientific evidence.
https://www.cell.com/neuron/pdf/S0896-6273(20)30431-1.pdf
“It is now well established that dysregu- lation of both the innate and adaptive immune systems occur in depressed patients and hinder favorable prognosis, including antidepressant responses.”
{kind=link}