Updates from MSF which highlight the level of mistrust and superstition amongst the infected population, where people hide their sick relatives from isolation wards and take them back to their village. We cannot exactly put a giant fence around the place (and not that this would be a reasonable goal anyway).
Do we invade these countries and force our will on them in order to prevent a humanitarian tragedy? What gives us that right? What gives anyone that right? To someone who is not sick, forcing them from their village, for forcing them to stay in their village violates their basic human rights, and yet it is for their own good, but if they don't believe that, what moral authority allows us to overrule that belief?
As you can see I struggle with the challenge of imposing a solution on these people, knowing that without aggressive actions tens of thousands, perhaps hundreds of thousands of them will die. While explaining to someone who doesn't understand the virus, or the danger, who undergoes forced relocation to a quarantine camp and is never sick during the outbreak, that they were in very real danger from this thing they do not believe in.
A creative solution would be to temporarily halt all regulations on anti-ebola drug development and let them experiment on any willing person in Liberia who wishes to receive treatment. The example of Banting and Best in the 20s is a great example of the enormous progress that can be accomplished if there is no regulation on medicine. These guys came up with the idea for extracting insulin from animals and injecting it into humans. They tested it out on willing patients, the first being a 14 year old, released the invention for use by the public and won the Nobel prize in the span of 3 years (1921-1923). That speed of drug development and testing is impossible today.
A good analogy of the present situation would be this. Someone is drowning in the river. You can use the military to prevent him from knocking any nearby bathers into the river as he floats down stream but don't you dare throw him something handy like a branch or a quickly improvised flotation device because that might help him float and it may not work and there would be lawsuits or regulatory violations! You can pay someone to swim after him and try and save him, but the stream is really rushing fast and they might drown too, but that's seemingly a-ok.
I realize the people of Africa are very poor and can't really afford the scale of production necessary. Perhaps your country would be willing to help out with a few million dollars, I'm sure this snake oil would do some good.
I'm all for effectively unlimited money from the first world to help pay for a response to this outbreak, but even if there was unlimited resources you can't just build up a whole medical infrastructure with the snap of your fingers.
Let's say this happens : http://en.wikipedia.org/wiki/Thalidomide
(First read about the advantages of the drug, then move to the crises. in particular the birth defects crisis)
And please don't just say that people knowingly took the risk, read the article first to see how that played out.
People won't accept the consequences of decisions made under duress (and this decision would be "death or we experiment on you". Decision to be made in an isolation camp, guarded by soldiers with guns), for obvious reasons, and this has been an accepted legal principle since a millenium before Jesus was born. You're suggesting just canceling it ? Really ?
What you're suggesting is a really, really, really, really bad idea.
Better-informed villages, towns, and cities have every right to refuse to admit, or interact with, individuals from superstitious villages. Self-defense is a powerful right, and I'd say it easily trumps a potentially infected person's right to visit a cousin.
People are free to die for their beliefs, whether such beliefs are true or not. But they have no right to make other people die with them. If push comes to shove, better-informed villages will expel all infected persons (preferably into quarantine centers, not into the jungle), post armed guards at every entrance, and either isolate themselves or only admit visitors from villages that have enacted a similar policy.
Unfortunately, it doesn't sound like it worked particularly well, considering the Plague still took a sizeable percentage of the human population at the time.
The prevailing attitude there seems to be "yes", but the difference is that in those cases the worst that could happen is people lose money, data and maybe their personal information gets leaked; whereas here, with Ebola, people will actually die. Not that I'm advocating either side of the argument, but it's something to think about...
I do my best not to be a knee jerk reaction person, but an airborne ebola strain, is beyond question a deadly deadly threat. Ebola has an incubation period, there is a period of time where you are infectious, before its obvious, and if airborne your very presence places anyone in the room with you now has 50/50 odds of living. This isn't SARS, this isn't Spanish Flu. This is quite possibly the closest we can get to a disease threat strait out of a zombie movie. I don't feel we should violate the human rights of everyone in that region, but this is one of those things where its squarely a "The needs of the many, outweigh the needs of the few or the one." scenario. So if the army doctor says "that guy has ebola, stop him from running away", I kinda feel (presuming an airborne ebola) that the situation may (depending on how far away he's getting, indoor or outdoor, etc) warrant lethal force.
Liberian President, Ellen Johnson Sirleaf to Barack Obama: "I am being honest with you when I say that at this rate, we will never break the transmission chain and the virus will overwhelm us"
"The dilemma" of invasion and whatnot is beside the point. The Liberian state is desperate. Johnson Sirleaf also recently fired 10 government ministers who had fled the country. Any nation with resources that wants to take over? The Liberian state would eager for the help. Things are that bad.
http://www.nytimes.com/2014/09/13/world/africa/liberian-pres...
One of Liberia's biggest newspapers recently ran an editorial claiming the Ebola epidemic was deliberately created by the US government. If that's the sort of paranoia that exists now, what do you think it's going to be like if thousands of Americans with filter masks and machine guns start flooding into the country? In addition to all the usual bad results, you're going to get a lot of people hiding and running - carrying the virus with them.
Statistics on mortality.
And while I'm pretty cynical as rule, it seems cynicism and despair at this point could actually hurt people.
The factors feeding into the Ebola crisis, and emerging from it, are sobering both in their interactions and how they tend to lead toward a fairly inevitable conclusion.
As for whether or not this is possible to avoid: human population and impacts on the world are unsustainable. Something is going to happen to bring numbers down. Voluntary population control, disease, starvation, war, social disruption, or other catastrophe, are pretty much the only real operators.
In that sense, yes, I'd argue that the general concept is pretty unavoidable.
I'm not saying Ebola (or this particular outbreak, or even necessarily disease) is "the one" and that the End Times have come. But it's a bit like an old-school video game. The challenges will keep coming harder and faster until we fail one.
This release from WHO sharply highlights this issue: http://who.int/mediacentre/news/ebola/8-september-2014/en/
Most of the infected cannot even afford to travel.
Somehow I don't believe that an action like this is possible in a democracy :/
- 1924-1925 smallpox outbreak and mass vaccinations in Duluth, Minneapolis, and St. Paul: http://www.mnopedia.org/event/smallpox-epidemic-1924-1925
- 1947 smallpox outbreak and mass vaccinations in New York City: http://www.virology.ws/2009/12/22/smallpox-in-new-york-city-...
Right, because it is not beneficial right now (it's not like there is oil in there) and we can always take action later when it gets closer and more serious.
https://lukoil-overseas.com/press-centre/7059.php
"The possibility of an airborne-transmissible Ebola virus is one 'that virologists are loath to discuss openly but are definitely considering in private,' wrote Osterholm. In its current form, the virus spreads only through contact with bodily fluids, he noted, but with more human transmission in the past few months than probably occurred in the past 500 years, the virus is getting plenty of chances to evolve."
The current rather high rate of transmission of the disease from one patient to another is alarming, and is perhaps preventable by better public-health practices aided by significant overseas funding, but if the virus haphazardly mutates into a form that spreads though more modes of transmission while still being as lethal, the world is in for a very severe challenge. As it is, the predicted number of cases by the end of the year will overwhelm several countries in the region where ebola is now spreading.
[1] http://www.cidrap.umn.edu/news-perspective/2014/09/experts-r...
https://donate.doctorswithoutborders.org
The health systems in these countries were already overwhelmed and under-resourced long before Ebola broke out, and the international governmental response has so far been alarmingly tepid.
Recent AmA with an MSF doctor:
http://www.reddit.com/r/IAmA/comments/2g79ip/i_work_for_doct...
Note that MSF has an excellent efficiency rating (~87% of revenue goes to program expenses, 11% to fundraising):
http://www.charitynavigator.org/index.cfm?bay=search.summary...
In particular, the history of events to date makes it clear it is not a case of the world doing nothing. Back in the spring, when there was reasonable hope that sending a bunch of foreign doctors could stop the outbreak, that was done - for a little while, it even looked as though it had worked.
Unfortunately, it didn't, by a long shot. Now WHO and MSF want to repeat that strategy on a much larger scale.
My opinion is that this is a very bad idea. The epidemic in West Africa not going to be stopped. That window of opportunity closed months ago, if it was ever open. If we send in thousands of doctors now, a large percentage of them will end up dead, and the epidemic still won't be stopped. It will be a waste of life, and at that, of the lives of trained doctors and nurses who will be all too soon and badly needed if the epidemic does start hitting other regions where the outcome would still be in doubt.
And no, sending in the military is not the answer. Not only does "it's for your own good" not morally justify aggression, but by further eroding the trust of the local population for authority in general and foreigners in particular, it would make matters worse, not better.
The affected area needs to be sealed off so the disease can't spread to the rest of Africa and the rest of the world. By all means airdrop medical supplies to Liberia, but don't for heaven's sake start sending hordes of doctors, soldiers and camp followers there to create more fodder for the virus.
So this new paper is projecting that Ebola deaths in Africa will be about as common as Malaria deaths.
I guess I'm trying to draw any conclusions or imply anything here other than life in Africa is pretty freakin' tough.
Unless the diseases start "competing" with each other. You can't really die of both. I don't know if the demographics of the two diseases overlap enough that this might happen.
1) We are due for another pandemic. If this one isn't it, there will be another.
2) Democracies run on public opinion. Right now everybody is riled up about some homicidal idiots in Iraq. This is off their radar. Hundreds of thousands of people die from some natural cause or another all of the time. It's not a huge spectacle on YouTube.
3) The enemy really isn't Ebola. Ebola is just the opportunistic pathogen that came along. The enemy is really weak governments with little or no public health systems, combined with very poor local sanitation practices.
4) There was a time when air-dropping in a thousand healthworkers with tent hospitals might have stopped this. That time is over. Now it's in the big city, and trying to control or service a population of several hundred thousand is beyond most any country's ability to project intervention.
5) If it doesn't go airborne and stay lethal, which is where the safe money currently is, we'll end up with hundreds of thousands or millions dead and it should burn itself out over the next year or two. That's the optimistic scenario. We have no reason not to believe that's the way it's going to play out.
6) If it goes airborne and stays lethal, we're in for a major shitstorm. But I really don't think second-guessing how we responded will be useful. There are different countries in the world. They have different governments. We do not have one world government, nor do most of us want one. That means that there are always going to be large pockets of humanity where something like this can take off. Structurally humanity is huge. Disease is going to be an issue for us for a long time.
What do you mean by this?
Did they seriously screenshot that image with a tooltip up?
No, R will stay the same. Or decrease as the population becomes more exposed.
So you want to send the military in? Do you have any idea of the size of the area in which you would have to deploy them, coupled with the panic their presence might cause, together with the issues which would be caused by militia factions which would inevitably arise to tackle what they would rightfully see as an invasion of their countries?
What did the UN manage to do after the Haitian earthquake that the Haitians couldn't have done themselves, besides introducing cholera to the region and nearby countries?
What African countries need to do is what they would have to do if there was no possibility of outside support. In this case it is not even a question of central government intervention when it is more a question of dealing with Ebola at the local level or county / village level.
Moving infected people to centralized locations for treatment means more travel and the possibly infected relatives and carers for the ill spreading the disease more, unless they are transported by specialist units. The process of travelling to report an infection and calling for a specialist unit itself carries the risk of the traveller spreading the disease let alone the person with the symptoms.
The only way to contain Ebola is to give the families or communities of infected people the knowledge, the drugs, the equipment and the protective clothing to they need to treat themselves and the economic support they will need when they are isolated, which needs to be done at a local level. That means sustained public education via television and video, protective clothing for carers and disease detection kits.
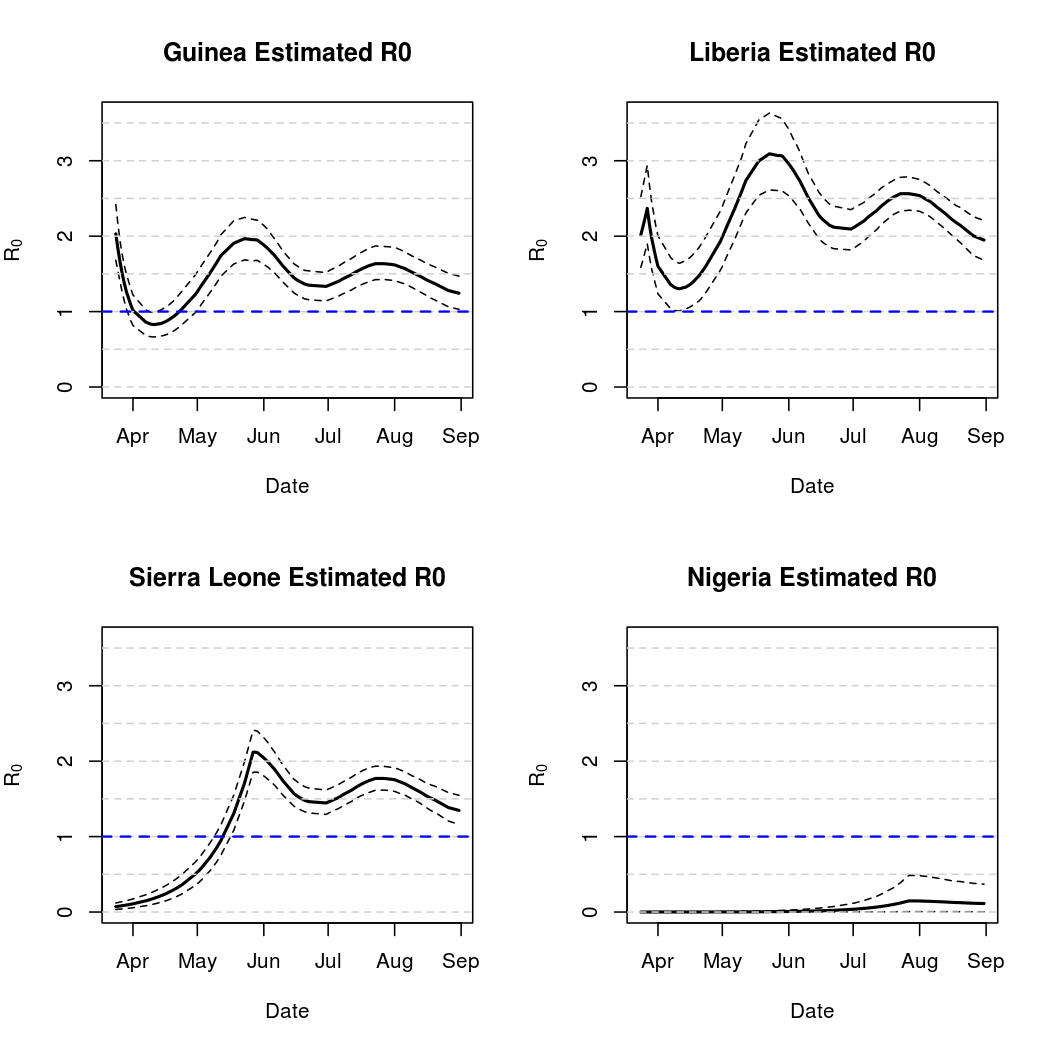
1) The article mentions the R0 of Ebola and claims it is between 1-2 in the current outbreak. Previous outbreaks of Ebola have been as high as 2.7. But this is relatively low compared to other diseases... the R0 of the Measles for instance is 12-18 (and nobody is really talking about the recent outbreaks in the US due to parents not vaccinating their children). Chances are, this rate would even be lower in the West because conditions in African slums and even hospitals are downright deplorable. Doctors aren't using suits or even gloves to examine patients, medical staff are reusing disposable needles, hospitals rely on family members to wash soiled linens because they don't have in-house cleaning services like western hospitals, etc. And don't forget that cultural norms are feeding the spread of the disease: well family members are observed to be sharing beds with sick loved ones in hospitals, people are practicing cultural burial routines of washing and in some cases kissing deceased loved ones, people are still eating the meat of things like bats and gorillas that are sick with the virus (and even found dead), etc. These are all things that just wouldn't happen in the West. People also do much better here at heeding the advice of the medical professionals - for instance, bodies of people who had died of Ebola would like be burned without concern for any regular traditions, without much complaint.
2) Part of the reason Ebola is so scary is the high fatality rate cited in articles: 50-90%. If you extrapolate to the entire planet, this sounds like it would be devastating to the human race. But is this the actual fatality rate? Western hospitals do a much better job of carefully monitoring patients and tending to every minor development. The main problem with Ebola isn't that the body can't fight it, it's that it kills you before your body can recover - the drastic difference in care between the West and Africa would likely make a huge difference in mortality. Make no mistake, this is a deadly disease, but probably not quite as bad as 50-90% in the West.
3) This article and others like it have shared the concern that Ebola could mutate into something transmissible by air. This would make the R0 of the disease skyrocket up into something that could quickly overwhelm Western medicine and very rapidly turn into something perhaps even more devastating than the plague. It's possible of course the virus could mutate in this way, of course, it's already believed that it can spread like this in pigs. One important thing to recognize is that Ebola in humans affects the liver not the lungs, which poses a barrier to being airborne. In addition, to become truly airborne, the virus would have to mutate it's outer coating to resist the drying effect of the air. So in order to become transmissible by air, it would have to mutate 2 different major adaptations and completely change everything about itself. The example I've read is that we don't worry about HIV becoming transmissible by air, and it is thought to mutate more quickly than Ebola. We've never observed any deadly virus change it's method of delivery, although of course airborne diseases evolved that adaptation in the first place.
None of these points mean we should sit back and do nothing. We need to help at minimum because of the following reasons:
1) People are dying and we can help them. With effective medical care, the mortality rate as mentioned in point 2 above should go down.
2) Ebola is destabilizing the region. This is already a region prone to state failure, corrupt and ruthless governments, etc. This disease could well cause wars in Africa, which in turn would make conditions worse and likely increase the fatality rate and the infection rate.
3) While there is a reasonable scientific case to be made against the unlikelihood of the mutation of the virus into airborne transmissible, it's possible and very scary. When considering the risks, we need to multiply the rather small chance against the rather large negative effect of such a change. We need to stop this to avoid this thing from becoming more deadly.
http://www.ecdc.europa.eu/en/healthtopics/documents/0905_pan...
Note the sharp jump as R_0 goes from sub-2 to over-2, which should not be surprising (hand wave about branch processes, light of a thousand suns, etc).
Over to someone better qualified to comment - is the present situation with Ebola taking us into a pandemic territory similar to 1918 H1N1?
I have seen this several places over the past week or two – is it actually true that people who survive Ebola are not at risk of re-infection? I can see where that might be true shortly after recovery (i.e., due to there still being antibodies in one's system), but how long would the immunity last?
Does that explain why people are not immune from the flu after having it once – the version they have antibodies to is not the same as the mutated version which circulates later?
It's available on iPlayer until Friday 19 Sept. 2014 http://www.bbc.co.uk/iplayer/episode/b04hcthj/
Someone's uploaded it to YouTube, although the last 10 minutes are missing https://www.youtube.com/watch?v=bjuQofIleOg
What I wonder is: why do they think it will stop? What's going to put a brake on the epidemic's explosion? This is not a world where a disease can burn itself out on the local level by simply killing everyone susceptible.
It is easily spread by sick people touching things (eg handle bars in the tube) which you then touch, before touching something that goes into your mouth. If Ebola came to the uk without major changes in behaviour it would likely infect millions of active, young people via London.
(It's easier to recognize a straight line on a log scale, than to distinguish an exponential line on a linear scale from a line that's "merely" quadratic, say.)
I guess there's a biological reason....
If these things are damaged (as they are when the virus is exposed to the atmosphere, or to enzymes in saliva), they're rendered non-infectious. So many details would have to change about the cells the virus targets, and the way that it enters them that I can't see how it would be the same virus, with the same pathogenic effect if it were somehow to become airborne. There are tradeoffs in everything, and viruses face them too.
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3498927/
> Piglets [with Ebola] were transferred to the room housing macaques in an open inaccessible cage system. All macaques became infected.
Yes there is a risk of mutation to transmit via air, but we have not yet seen it. We have merely proven that 'shit happens' and 'ebola is dangerous'.
[1] http://www.aidsmeds.com/articles/life_expectancy_1667_24972....
I'm afraid some people either think this is a game, or just an opportunity - since most of the worlds problems today stem from overpopulation.
Why do you think that most of the world's problems today stem from overpopulation? What problems?
If you're talking about hunger, that's demonstrably false. There is plenty of food produced to feed the entire population. Even African produces plenty of food to feed itself. Famine occurs in times of war and natural disaster, or other great upheavals. Most of the causes are man-made and have nothing to do with overpopulation.
I'm not saying all of these are correct in an absolute sense, just that population certainly plays a role.
Uh - collapsing ecosystems? More to the point, encroachment of humans into wilderness areas which harbor viruses? The biggest 'man-made' issue here is more 'man': mindless reproduction and consumption without any regard to the future.
“I’m not afraid of nuclear war. There are 2.7 billion people in the world; it doesn’t matter if some are killed. China has a population of 600 million; even if half of them are killed, there are still 300 million people left. I’m not afraid of anyone.”
http://www.theepochtimes.com/n3/4758-maos-nuclear-mass-extin...
BTW Ebola propagation maps I've seen show China having the slowest penetration rate of all nations.
In general do mutations follow probability distributions that are known?
And then let's say someone wanted to cause mutations that would make it airborne. Could they do it?
In some ways, yes. Substitution matrices[0] describe how likely it is for an amino acid to mutate into another amino acid. However, they are generalized descriptors. At the same time, PWMs[1] describe how the probability of any given variant (mutation) is in a specific sequence, and are created by analyzing all known homologs (similar sequences) of that sequence.
However, the number of mutations required for a virus which is incapable of becoming airborne is probably large and definitely unknown. I'm not an expert in virology, but I believe that there are two requirements for a pathogen to become airborne:
A. It must infect and replicate in an area of the body capable of generating aerosols (generally, the respiratory system, like Influenza and Tuberculosis).
B. It must be good at surviving in aerosols- I believe this requires specific environmental adaptations and the right surface proteins and sugars.
I believe that Ebola meets neither requirement (especially the first), and you could see how meeting both would require not just large physical adaptation, but also a complete change in the virus' life cycle in the host.
>And then let's say someone wanted to cause mutations that would make it airborne. Could they do it?
I think in general it would be easier to start with an airborne virus, and make it deadlier. I'm not an expert but this BBC article[2] quotes that a deadly virus has never been observed to change their vector of infection.
0. http://en.wikipedia.org/wiki/Substitution_matrix
The way that South Africa dealt with their AIDs epidemic (from a western perspective, true head in sand activity) is a case in point: despite many aggressive offers of help from western governments, the South African's continued their denial. To make a change would have required going against the government policy of the time. This is viewed legally as an invasion by an outside force.
The articles I read describe the problematic issues being; a lack of running water in existing clinics, a lack of medical supplies, a lack of clinics and notably a lack of food everywhere - patients are escaping isolation in efforts to find food.
Liberian officials have pleaded for help in fairly abject terms (one official mentioned the possibly of nation ceasing to exist - I think that means they're worried). The details of what Western nations have done so far is fuzzy but it seems like there not been a sufficient rush to deliver these acutely needed supplies.
Sure, once the existing clinics have food, supplies and running water, parachuted in field clinics sound grand. There's no evidence I've seen that the Liberians would refuse these.
Many African nations have a history of dealing with problem regions, such as regions that have the wrong politics, tribal affiliation, or religion, by going in with their military and killing everyone in sight.
What are the chances some of these countries might decide to deal with the problem of Ebola infected regions that way? Especially regions where superstition or ignorance lead the people there to avoid treatment? If the rest of the world waits too long to come up with a solution for the problem, I fear we may see a lot more deaths from this than just those who are killed by the Ebola virus directly.
Attempting use "force" to seal off the area, is perhaps the single most effective way to lose all control of this disease, and see it spread to hundreds of thousands, if not millions of people who (quite reasonably) decide to fight back against such an activity.
Careful Training, use of locals who have developed immunity, massive injections of beds, medicine, and supplies, can have a huge impact, and keep this current epidemic under control
By contrast, the strategy I advocate has thus far been working.
Nigeria? Cut travel to the affected area. One idiot had slipped through, causing an outbreak. Because it was only one small outbreak, it was possible to contain it.
Senegal? Same. Tougher problem because it has a land border with the affected area. In response, citizen groups have been supplementing the security forces, patrolling the border and turning back people trying to enter the country, thus far successfully.
Ivory Coast? Cut off travel from the affected area. Thus far, no Ebola detected.
Do you believe in results? I advocate abandoning the strategy that has been proven not to work and focusing on the strategy that has been proven to work.
The reason things got out of control is that the world relied on charitable organizations to fix things, but the wonderful folks at the MSF were quickly outgunned.
With that being said it varies a LOT between different countries for exactly the reasons you mention. My initial work shows a lot of heterogeneity:
http://grantbrown.github.io/Ebola-2014-Analysis-Archive/Sep_...
I agree wholeheartedly with your last three points. Also, from the looks of things the cheapest and most effective time to tackle the disease was months ago. The second cheapest and most effective time to try to stamp it out is as soon as possible.
P.S. The ProMed daily digests are some of the best and most comprehensive updates on this situation I've seen:
You only need a handful propagating a suddenly airborne version of the disease to London, New York, Paris, Tokyo, Beijing...
Most is not good enough.
The areas currently buckling under Ebola have not been the regions of Africa most affected by famine in the last few decades, most of which are in the Sahel and Horn of Africa. And which were caused by political problems. Other than that, I'm not sure what this means.
>"Global warming" - we could reduce emissions by reducing population without changing the per capita energy consumption.
This would be true if you reduced population in the West and in Asia but the energy and food consumption of Africa is absolutely minuscule compared to the rest of the world.
See the references in my other post:
https://news.ycombinator.com/item?id=8320473
>Strife in the middle east?
Israel has a relatively low birth rate.
I don't think the people speculating here understand how bloody military quarantine imposed by a foreign power could be - however well intentioned - compared to the mere 2,200 people who have died of the disease so far.
Send in a U.S. Marine division of 20,000 people (or maybe make it a "coalition" and send in a few hundred European troops as well to, ahem, share the burden) and tell them that they need to direct some people from one place to another, keep some people penned up, keep all these people fed, keep them from doing anything unfriendly to the nice doctors in the space suits, and everyone who resists - resistance here includes rioting or just not being able to follow instructions because, you know, the troops don't speak the language - needs to be taken into custody with that legendary marine gentleness while being treated as a potentially lethal disease carrier. Keep the troops mindful that if they err on the side of laxity they could get a disease that might cause them to die bleeding from their bodily orifices.
Multiple massacres should be the expected outcome of such an operation. The projected cost of the disease needs to pretty horrible before it becomes worth contemplating such a high-risk, low-reward action and we'd want to exhaust all other means of supplying these countries' civil authorities with what they need before we took such a step. We haven't done that yet.
Guns down.
Yes. There are many strains of Influenza, immunity to one strain doesn't necessarily confer any immunity to another strain.
However, Ebola mutates much less rapidly that Influenza.
http://web.stanford.edu/group/parasites/ParaSites2012/Lassa%...
http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5005a1.htm
Looks like there were about 10 new cases/day at its peak; the current outbreak is at 150/day.
A couple things stood out to me:
Fourteen (64%) of 22 health-care workers in Gulu were
infected after establishing the isolation wards; these
incidenses led to the reinforcement of infection-control
measures.
During the 4-month outbreak and response period,
approximately 5600 contacts in Gulu District were under
surveillance for 21 days by approximately 150 trained
volunteers.And to the point, we've never successfully "beat" GI because the stakes were never this high.
More opportunities to evolve doesn't mean a rapidly mutating virus, relatively speaking. It may be mutating faster now because of more opportunities, but the virus still mutates orders of magnitude less rapidly than influenza.
Today, outsiders can airlift food, clean water, and medical supplies to any isolated village that asks for help. So let's stop wasting resources on people who don't want to be helped, and focus on people who actually are desperate for help.
No, not every individual knows or understands this, particularly in primitive areas. But the global system as a whole does.
As for the Black Death, there are instances of specific villages or households (or castle-holds) who sealed themselves off and had sufficient stores to see themselves through the plague.
I understand the distinction you are trying to make, but I think what you call "growth rate" would actually be "growth acceleration".
...has nothing to do with overpopulation and everything to do with tragedy of the commons and destructive corporations. Brazil's rainforests would be cut down regardless of what the population of Brazil was.
>The biggest 'man-made' issue here is more 'man': mindless reproduction and consumption without any regard to the future.
And it's stunning to see the charge of "mindless consumption" being thrown at areas with the highest population growth like Africa, when their rates of energy and food consumption cannot even compare to those in the developed world. They're miniscule [1][2].
1. http://en.wikipedia.org/wiki/List_of_countries_by_energy_con...
2. http://en.wikipedia.org/wiki/List_of_countries_by_food_energ...
I'm writing a dissertation on infectious disease spread, and your comments strike me as uninformed and harmful. The time for massive action is now, and pipe dreams of impossible (and downright inhuman) international quarantine cordons only confuse the issue.
Or perhaps we should ignore the best advice of both the medical and epidemiological communities and throw our effort behind an impossible and inhuman military containment scheme...
And yet, when something manages to hit us on an emotional level we falter.
What Afforess said is a statement of fact and relevant to the discusssion. Thus it's a valid counterpoint.
You may not like it and you may not agree with it .. you may even discard sprituality as a whole .. but none of it makes the satement any less true.
So given the problem of doing something about a disaster, trying to keep all the different belief systems happy at the same time will just stop you from doing anything. You can't keep all the different belief systems happy when there isn't a disaster and lives to save, trying to do it when there is seems to be just setting yourself up to fail from the outset.
Also, given the context of disease, stopping it spreading is not a wholly altruistic act. This is about self-preservation as much as anything else and most of the world's religions are pretty clear on what you are allowed to do to others when the tribe is threatened. The religious reaction to this in many cases would be mass slaughter.
Australia and the Netherlands had a similar issue with the downing of the Malaysian Airliner in Ukraine. In this case, the Ukrainian government had to pass legislation to allow armed Australian and Dutch military to support inspectors. They were just 'inspecting', not creating forced closures of specific areas, forcing burials, witholding care, etc all under significant armed guards.
The present situation on the ground (and the lack of 3rd party government level interaction) is largely a result of weak leadership by the UN. The better question is why the UN hasn't taken ownership of the outbreak?
Liberia does have Liberian burial specialists now, who do what you describe and it indeed is probably the most awful job in the world. Indeed, the Liberian government, with varying levels of competence, has attempted to do most of what you describe. Essentially, there's no evidence, no indication that the Liberian state would resist UN or US aid but also very little evidence of such aid. If anything, the Liberian government has done some stupid impingements on rights itself (quarantining the entire poor sector of Monrovia for example).
Yes, the Liberian state is already taking desperate and extreme measures but when most clinics without running water, their options are limited. I'm sorry, this stuff make me so angry I could ask what it says about you and your ilk when you're so eager solve things with guns that you don't notice that lack of food and water is the primary problem?
Obama some announcements about military assistance but I've read not article about anything materializing.
Seriously, we're talking pretty well unprecedented disaster - the response has been much than even the response to "typical" third world disasters, much less than the response to the Haitian earthquake for example.
It is not official action that the parent commenter is referring to. Individuals themselves could treat actions they see as counter to their religion and belief as very hostile.
Btw, as far as I see the only one on the high horse in this comment thread is you.
Not all religious sects have an afterlife and some, like Calvinists, believe in predestination, so nothing you do affects where you are going anyway.
edit - The position of respecting other beliefs as the number one priority is basically saying that it is better to let someone die than offend them. However from a religious perspective you wouldn't normally give a shit about offending other people's beliefs as other religions are generally regarded as heresy. There are exceptions, such as the Baha'i, but generally the idea of trying to respect all beliefs is largely a secular position.
http://reliefweb.int/report/democratic-republic-congo/update...
"One of the patients hospitalised at the HGR Boende had managed to escape before being recovered by the services deployed to the field."
The guy escape because he was starving - he went immediately to the market to buy food. If he had food in the isolation ward, that wouldn't have happened (or would be a good deal less likely).
And uh, the idea of shooting people infected with Ebola shouldn't be first or second resort considering you would be straying their infected blood over a significant area. Not to mention guaranteeing no else would want to be treated, etc.
(In case you're dense, just like the last time we tried to bomb a country into freedumb.)
edit: and just who vets the people/companies who get to offer drugs to desperately ill people? Does anybody with $1k to buy needles get to make a sign and advertise curative injections? I'm sure glibertarian idiots will say it was a freely made choice, but choices made while infected with ebola (or even scared of being so infected) aren't freely taken, not to mention the asymmetric information.
Please avoid making personal attacks like this on HN.
As a mostly libertarian-minded person myself, the height of compassion is to allow dying people to reach out for any hope out there.
Cruelty would be to prevent people from attempting to save their own lives "for their own good"; especially when no alternative cure is being offered by the politicians and bureaucrats making such life-impinging decisions.
Yes, the quacks and charlatans will try to take advantage and they should specifically be combatted. That doesn't mean that people should not be able to make decisions about their own lives.
Look at the scientists who were helping fight Ebola in Africa. When they discovered they were infected as well they had the chance to take a new treatment and they took it. And they recovered.
The question of who decides is important, I'm not saying it should be overlooked but the possibility is not even there for those who actually want to take it desperately. And no need to throw the "libertarian" word for everything you disagree with, we are talking about having choice here.
It's a calculated risk, sure, but I don't think the Thalidomide example is particularly relevant.
It's very relevant. It shows that people are too willing to take risks with major unknowns. Where do you make the cutoff with your drug experiments? Only people that are certain to die? People with high exposure risk? People that are having difficulties recovering? Any selection you pick there is completely arbitrary because you don't know the potential downsides to the experimental stuff you want to try.
I don't know where you make the cutoff, but I'm comfortable saying that its somewhere below having a disease with a 50% mortality rate in under 14 days. I'm pretty much okay taking any risk at that point.
I agree that it may be an idea to look at trying some of the experimental treatments, however given there is a 50% chance of surviving with palliative care and that we know how to stop it spreading given the resources, I am not sure that turning the situation into an unregulated free-for-all for every quack looking to make their name will really help matters.
The question is whether to suspend normal precautionary procedures during an extraordinary situation, not whether to ditch normal precautionary procedures which exist for very good reasons (see the Elixir Sulfanilamide disaster for why):
http://www.fda.gov/aboutfda/whatwedo/history/productregulati...
You're rightly concerned for the possible side-effects of using untested treatments on people during an emergency. But flip the question around: who's liable for not deploying an available experimental treatment that is later determined to work, but only after tens of thousands have died while it sits, unused, on the shelf due to lack of test data?
At the same time though, we need to realize that this is primarily about protecting the health professionals and care givers, and only indirectly the sick. (The sick will of course indirectly profit from professionals being just that - professional, but only in the "long term".)
We should have no delusions about willingly letting people die, in the name of professionalism, just to have a clean concience and the ability to claim to have done nothing wrong.
No one, that's exactly the point.
There's no way to sort out misdeeds, eg, fake cures from real attempts if we lift the normal trial and liability procedures. No one would use untrialed drugs if they had to take the full liability.
So the reality is that there is no good way to send only useful drugs there while skipping the filtering process.
If you're okay with some people being poisoned or lied to for money in the hope that some people will get a real drug, then we could make that work, but I'm not sure we want to go down that path.
I'm ready to assume that medics treating an emergency epidemic are unlikely to knowingly turn to quack remedies -- homeopathic or bogus ones -- as opposed to items like ZMapp, a monoclonal antibody treatment by a well-regulated pharmaceutical company that just happens not to have been approved for human clinical trials yet.
http://www.cdc.gov/vhf/ebola/outbreaks/guinea/qa-experimenta...
Furthermore, let me add that conducting a randomized controlled clinical trial (for effectiveness and safety) when dealing with a pathogenic infection with a > 50% fatality rate is arguably unethical: you can collect data on clinical applications and apply a retrospective control sample of patients to determine whether it improved the outcome where it was used, but withholding a potentially effective treatment becomes extremely problematic under some circumstances -- the historic classic example was zidovudine for HIV, which was rushed through human trials into use in just 27 months because it was the first effective treatment for a then-100% fatal disease (HIV). (Some of the double-blind trials were short-circuited when it became apparent that continuing to alternate patients with placebo controls was likely to be injurious.)
We all love silver bullets and magic serums, but the real answer here is to get the basics right. There are major improvements that can happen in sanitation, medical care, keeping quarantines effective, proper handling of the dead, etc. A lot of major epidemics were stopped in the 1800s and early 1900s with these kind of things, Ebola can be fought in many ways without inventing a drug.
Solving the crisis on a large scale isn't really a "medical" challenge in the normal sense, it is about logistics and resources and public trust in government & doctors.
I think that if you were yourself in such a situation, with any incurable disease, you'd see the world in a different way. It's always easy to talk about things that do not concern oneself directly. And again, right NOW, Cancer patients have that choice, so why not others?
I don't understand the propensity of some to demean "hey, there's a serious immediate problem, let's do everything we can to help" with "but it might (with minuscule odds) go horribly wrong! therefore we can't let anyone do anything that's not established best-condition status quo!" With that mindset, it's a wonder such people ever drive to work (you might die in a horrible flaming carbecue!).
Statistical prioritization matters. Just because there isn't a perfect solution doesn't mean there isn't a better one.
And of course the deal is going to be that you take full responsibility for the risk. In other words, if something like that happens, you get zero assistance, not even from any health insurance you already have.
> I don't understand the propensity of some to demean "hey, there's a serious immediate problem, let's do everything we can to help" with "but it might (with minuscule odds) go horribly wrong! therefore we can't let anyone do anything that's not established best-condition status quo!" With that mindset, it's a wonder such people ever drive to work (you might die in a horrible flaming carbecue!).
Short answer : because it's happened before.
I would also argue that given history, the risks of unknown treatments having major side effects are significant (let's say ~15-20%). The risks of major side effects on pregnancies and later offspring are even more significant (20-40%).
So those odds are not that minuscule and there are going to be victims.
Your attitude stems from the idea that seems to be propagated a lot these days : that science and therefore medicine can fix anything, any disease. That was almost true for a short period at the end of the 70s. In the 80s we found several diseases became fully resistant. Now the counter of completely incurable diseases is in the thirties, and rising fast. Old, well-known diseases are coming back, untreatable. Tuberculosis, pneumonia, dysentery ... all have MRSA variants. And that's ignoring a lot of viruses. Rabies, HIV, Hep C, MERS, Avian flu, Pig flu, ... all of which are essentially untreatable.
The point the CDC has been making for ~20 years now is that ~3 decades ago "net-"scientific advancement against infectious diseases stopped. There were advances, but diseases advanced at roughly the same pace. 2 decades ago we started losing ground and in the last decade we've been losing ground like never before.
And of course we're completely focusing on the wrong solution : don't use medicine anymore ! Great, but that ship has sailed, adaptation has happened and it's generally too late. There have been studies on how long these adaptations last, and how long we'd have to wait if we stopped treating ill people. The timeframe is in the centuries.
What do you do when something with 51% mortality in 15 days comes up? And then something with 49% in 13 days .. where do you draw the line? And what do you do when people continue to cry out?
I'm not sure if you are aware but in Africa right now people infected are actually going to see the quacks and shamans because they have no other option. Maybe it's time to think about providing them with something that has more scientific ground to actually work.
Exotic cures are sure exciting to talk about. But for a disease that can be stopped cold in its tracks by washing hands and effective quarantine, they're having a bucket of trouble accomplishing anything. Maybe its a little blue-sky to be adding complex drug protocols to the plan.
Yes, there will be victims. No, I don't subscribe to "science/medicine can fix anything" - don't put absurd words in my mouth/fingers.
Balancing those problems vs BEING DEAD, I'm irritated that you'd deny me the former option.
I've been dead once already; may the fleas of a thousand camels infest the armpits of he who would give me little choice but do it again.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}